Publications IPH Magazine IPH Magazine, issue #14 Architecture Regulations for Healthcare Facilities in Brazil

- Current Hospital Master Plan
- Architecture Regulations for Healthcare Facilities in Brazil
- How Hospital Rooms Went from Airy Temples to "Inhuman" Machines
- The healthcare hub
- Santa Casa de Misericórdia de São Paulo: A hospital architectural heritage
- How Architecture Has Influenced the Promotion of Hospital Hotel Services and Humanization
Architecture Regulations for Healthcare Facilities in Brazil
Antonio Pedro Alves de Carvalho













Brazil has one of the most advanced
regulations concerning Hospital Architecture, which should not be overlooked,
since it can be perceived in the quality of the spaces within healthcare
facilities.
Current regulations, however, result
from a lengthy evolution that began in the 1940's with the hiring of architects
by the Special Service for Public Health (Serviço
Especial de Saúde Pública - SESP) - an agency created by the Ministry of
Education and Health - that received American help to implement basic
sanitation in areas that produced raw material that were essential for war,
such as rubber, in the Amazon, and iron ore and mica in Vale do Rio Doce
(RENOVATO; BAGNATO, 2010).
Unlike laws and decrees whose mainly attributes are punishment and
behavioral orientation, regulations must stand up for their instructive and advisory
role, they do not have the power to suppress. Considering this point of view, we cannot study
the regulations concerning healthcare facilities without paying close attention
to the initiatives that enable teaching and imparting the knowledge concerning
the topic.
Writing and publishing regulations
will not be enough. Additionally, it is necessary to publicize and update it, since
the criteria adopted once may briefly become outdated or even wrong. The
evolution of regulations concerning healthcare infrastructure clearly shows the
important role of technical education, teaching and research as basic
guidelines.
From the establishment of Padrões
Mínimos Hospitais, by SESP (BRASIL, 194?), which was inspired by the
American publication Elements of the General Hospital (USA,
1946), up to our current regulations, we can perceive the leading aspect
that guides both creation and impartation of such regulations.
At present, there are discussions
concerning changing such regulations; and we would not go too far to emphasize
the need to debate the process of continuous maintenance of regulations that
must be implemented, assuring the educative role of such document.
Elements of the General Hospital
We may consider the publication of Elements of the General Hospital (USA, 1946) (picture 01) - published by the American Health Department - as the great source of inspiration for architects that work
with SESP to design the first guidelines concerning the topic.
Picture 01: Cover sheet of Elements of the General
Hospital (USA, 1946).
We can see that this book
offers an illustrated guide of plans for hospital facilities with thorough dimensions,
including a detailed list of furniture and equipment. They provide no other
written orientation, suggesting that the book, in fact, is a result of studies
undertaken by architects specialized in hospital planning to provide other
colleagues with the information necessary for each activity.
Picture 02: Example of a plan found in Elements of
the General Hospital (USA, 1946, p.20).
By providing detailed dimensions for every room, as well as the design of thorough plans for unities, their intention is to offer an instrument to guide those who would not have the time
or support demanded to project and execute hospital unities (Picture 02).
This brochure consists exclusively of drawings, which
are architecture suggestions for ambulatory and diagnostic facilities, surgical
department, admissions and general services; apparently considered the most
important areas of a hospital.
Padrões Mínimos Hospitais
SESP had acted upon several
healthcare and rural sanitation programs until it was shut down in 1990. One of
its greatest improvements, at the time, was sending professionals to the US for
post-graduation courses. The field of architecture gained with the exchange of
knowledge, which led to the creation of the hospital architecture sector.
Willing to guide the consultancy for
the design of small hospitals, SESP published Padrões Mínimos Hospitais
(BRASIL, 194?) (Picture 03), a 23-page book with models of architecture plans resembling the Elements of
the General Hospital (USA, 1946).
Picture 03: Cover of Padrões Mínimos Hospitais (BRASIL, 194?)
In the introduction of the book, the
head of SESP at the time says:
Since the engineering department at SESP implemented an architecture department, we thought convenient to assemble, for our own use, a guide that brings the modern guidelines recommended for small-size hospitals. Therefore, making the method of planning, studying and conception of the project for the hospital unities that SESP would build in rural areas more comprehensible, and at the same time assuring the necessary uniformity regarding standards of construction and basic equipment of the facilities. (BRASIL, p.3).
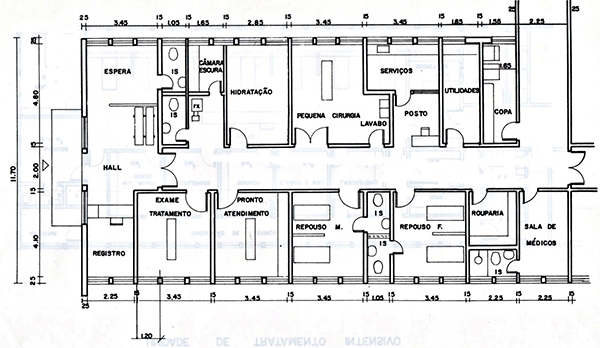
The book presents architectonic
solutions in graphic scale of several unities inside a hospital, apparently based
on architectonic projects concerning 50 and 100-bed buildings. By thoroughly listing
furniture and equipment that could be used for each space, the book presents
them in a way that could set the example for technical solutions. (Picture 04).
Picture 04: Example of a plan from Padrões
Mínimos Hospitais (BRASIL, 194?, p. 9)
The publication may be considered the
foundation of all legislation concerning the architecture for healthcare facilities
in Brazil and, graphically, it served as model for what was published
afterwards.
We can see the resemblance
between the Brazilian book and the way the Elements
of the General Hospital (USA, 1946) presents schematic plans, aiming at
guiding those who work with health infrastructure. We cannot overlook the fact
that in the beginning of the 20th century, the doctor-manager was the main
responsible for the projects in health unities. Up to the 1950's, the courses
concerning infrastructure in health facilities were related to hospital administration,
and, most of the time, were attended by doctors. Some doctor-managers, like Odair Pacheco Pedroso
(1909-1981) and Ernesto Souza Campos (1882-1970), were known for advising
projects to build hospitals.
The first event aimed at training Brazilian architects
to project healthcare buildings was the I Curso de Planejamento de Hospitais
(First Course for Planning Hospitals), held by IAB-SP, in 1953.
First Course for Planning Hospitals, held by IAB-SP
This was a pioneer and
intensive course held between the 13th and 17th of April 1953, by the Instituto de Arquitetos do Brasil,
Departament of São Paulo, and it was organized by the Comissão
de Planejamento de Hospitais, IAB-SP, a commission for planning hospitals that had the architects Amador
Cintra do Prado, Jarbas Karman and Rino Levi among its members.
It was an interdisciplinary event,
attended by doctors, nurses, engineers, architects and managers. Some of the
classes were fully recorded into a 528-page publication that became reference
in the topic: Planejamento de Hospitais (IAB, 1954) (Picture 05).
Picture 05: Cover of Planejamento de Hospitais (IAB, 1954).
The book was organized in twelve
chapters representing the topics presented by specialists in their lecturers:
I) Planning and Administration; II) Nursery; III) Radiology; IV) Physical
Therapy; V) Surgery; VI) Obstetrics; VII) Pharmacy; VIII) Ambulatory; IX) Laundry;
X) Laundry and Kitchen; XI) Research concerning hospitals; XII) Wrap-up.
It was during this course that the
architect Jarbas Karman suggested the establishment of the Instituto de Pesquisas Hospitalares (IPH), which, up to these days,
has the important role of encouraging researches and studies concerning
hospital infrastructure. This course represented a milestone in the studies of
hospital architecture in Brazil, by presenting to the community of health
professionals a new specialty within architecture, pointing out to the need of specific
knowledge that every professional working with architectonic projects for
health facilities should have.
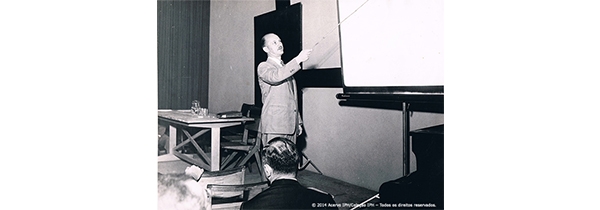
A great number of the lecturers presented in the course deserve special recognition. The architect Oscar
Valdetaro, from SESP, talked about the functionality of the several unities
within a hospital. The architect Jarbas Karman delivered a lecture on the
surgical department and the material and sterilization unit. This text can
still be considered one of the most important ones concerning this topic. (Picture 06).
Picture 06: Jarbas Karman delivering his lecture on surgical department at the First Course for Planning Hospitals, held by IAB-SP, in 1953 (IAB, 1954, p. 175).
The doctor Odair Pacheco Pedroso talked
about the ambulatory unit, the professionals and technicians needed to design
the project of a hospital and about planning a hospital under the
administrator's point of view. The architect Rino Levi delivered a lecture on
planning a hospital under the architect's point of view. The architect Jorge
Machado Moreira shared a general viewpoint concerning hospital architecture. The
architect Roberto Cerqueira César discussed the flow and means of communication
inside hospitals. Therefore, we can notice that this course gathered a remarkable
academic group that delivered content of great value, representing a milestone
for Brazil's health infrastructure.
The publications we have mentioned so
far were cutting-edge and inspired the first set of comprehensive regulations in
the country: the Projeto de Normas Disciplinadoras das Construções
Hospitalares (BRASIL, 1965).
Projeto de Normas Disciplinadoras das Construções Hospitalares
In 1965, the National Health Department
of the Ministry of Health in Brazil published the Projeto de Normas Disciplinadoras das Construções Hospitalares
(BRASIL, 1965) (Picture 07), written by the architects Oscar
Valdetaro and Roberto Nadalutti, advised by the doctor Henrique Bandeira de
Mello. In this publication, we can see more drawings of unities as well as
theoretical explanations for the projects, therefore meaning a great evolution since
SESP's book: Padrões Mínimos Hospitais (BRASIL, 194?).
Picture 07: Cover of Projeto de Normas Disciplinadoras das Construções Hospitalares (BRASIL, 1965)
IAB's chairman wrote the
introduction for the book, drawing attention to its informative style and emphasizing
that: "The current work represents an attempt to promote guidance for hospital
constructions, although not imposing strict instructions." (BRASIL, 1965 [s.p.]).
The book is divided into the
following chapters: Hospital terminology; Hospital: concepts, definitions and
classifications; Preliminary information for planning; Minimum Functional Programs;
General guidelines for specialized hospitals.
The concept of Hospital
Network is introduced by establishing a hierarchic matrix of service, as
follows: Base Hospital, District Hospital and Integrated Health Unit.
The core of the book is item
4, Minimum Programs, where plans (Picture 08) and tables, concerning minimum
space and area, and explanations of various types are displayed, such as: "Whenever
there is an emergency department, it would be convenient to have a radiodiagnosis
installation as near as possible." (BRASIL,
1965, p. 46).
Picture 08: Example of a common plan at Projeto de Normas Disciplinadoras
das Construções Hospitalares (BRASIL, 1965, p. 93)
This book guided the
construction of health facilities nationwide until 1974, when the Normas do
Hospital Geral (BRASIL, 1974) were edited.
Normas do Hospital Geral
The first regulations for hospital
infrastructure in Brazil - Normas do Hospital Geral (BRASIL,
1974) - were the result of decades of dedication and study of a group of
architects and engineers who were truly interested in the topic (Picture 09). In
the introduction, we find the following observations:
The regulations in this book were established by the Coordination of Medical and Hospital Assistance of the Ministry of Health to ensure that proper plan, project, construction and installation may enable the General Hospital to provide an efficient, safe and economic service.They aim at guiding architects, engineers and hospital advisors, however not imposing limits on architectonic innovation and building technic. These regulations provide, therefore, minimum requirements to plan, build, remodel or expand the General Hospital of any capacity and location within the national territory. (BRASIL, 1974 [s.p.])
Picture 09: Cover of the book Normas do Hospital Geral (BRASIL, 1974).
Its structure was less oppressive than
the one found in Projeto de Normas Disciplinadoras das Construções Hospitalares (BRASIL, 1965), since it did
not present imposing tables. Minimum areas were established through an
explanatory text and only for spaces of greater importance. The advising plans
were redesigned and organized as a supplement of the book called Estudos Gráficos (Graphic Studies) (Picture 10), which was introduced by the observation: "The graphic studies in this supplement, concerning the regulations, aim at producing
evidence of the minimum area suggested, unpretentiously. More satisfactory
solutions may be found, especially if there is more area available" (BRASIL, 1974, p. 150).
Picture 10: Example of "graphic study" from the book Normas do Hospital Geral (BRASIL, 1974, E.G. 13).
The associates for this book were: Hélio
Múller (Head of Architecture at the Division of Engineering and Environment
Sciences of Fundação SESP, associate at the publication of Padrões Mínimos Hospitais (BRASIL, 194?); Sylvia Caldas Ferreira Pinto (Head of Technical Orientation at the Healthcare and Hospital Coordination of the Ministry of
Health); Maria Torres del Negro Lima (Head of SOT's Engineering and
Architecture Department); and Léa Barbosa Baião (SOT's Architect). This
publication did not prevail for long, since, in 1977, the Ordinance 400/1977
(BRASIL, 1979) was edited.
Ordinance 400/1977
The Ordinance 400/1977 (BRASIL, 1979) was
a revised edition of the regulations that had been published in 1974. However,
the Ordinance had a clear imposing style, presenting tables with minimum areas
for each section and a graphic division with technical explanations and
examples of projects - some of them that had already been used in previous
regulations. The Ordinance was firstly edited in two volumes, the first one brought
only the tables and the second one had detailed explanations about the hospital
unities and sample plans (Picture11).
The Ordinance 400/1977 has guided inspections
and projects of hospital unities for about seventeen years. It became a rigorous
tool, therefore encouraging an extreme inspection system by the Health Surveillance
Agency, which would not admit big variations
concerning the established minimum areas. Obviously, there were several
architectonic solutions reproduced nationwide. Replicating the same solutions from the Ordinance would
guarantee that the project would be approved by the Health Surveillance Agency,
which was what inspectors from financing
agencies required.
Picture 11: Cover of Ordinance 400/1977 (BRASIL, 1979), volume I
The tables presented minimum areas with
inflexible strategies for hospital unities that would be acceptable for small
and medium-size hospitals. There were two sets of information: one valid for
hospitals with up to 50 beds and the other for hospitals with up to 150 beds,
besides some extra information. Hospitals with more than 150 beds were
considered exceptional and would have to be specially analyzed.
There was an introduction prior to the
tables, which covered: I-Physical Terminology; II-Proper Location; III-Indoors
and Outdoors Circulation Areas; IV-Built-up area. The second volume was more
informative, hence explaining the administrative work of the hospital and
providing project premises. It kept several technical orientations from the previously
regulation, which were valuable to study projects of healthcare facilities,
like the observations concerning location:
There must be a study concerning special conditions for the location of the hospital and choice of land, aiming at:a) Proper water supply in quality and quantity, at least 500 liters a day and by bed. Availability of sewerage and Rainwater harvesting systems, as well as electricity, telephone and gas systems.b) Proximity to the city center of the community at which the healthcare facility is aiming, there must be access roads and means of transportation.c) Only up to 50% of the land must be built on, considering further extensions [...] (BRASIL, 1987, p.13).
We cannot overlook the fact that, at the time, the study of healthcare
facility infrastructure was at its initial stage, therefore, publications in
Portuguese were rare to come across. In 1987, the Ordinance got a second
edition, in just one volume (Picture 12).
Picture 12: Cover of the second edition of the Ordinance 400/1977 (BRASIL, 1987).
The plans presented followed the 1,2x1,2m
modulation and there was indication of basic furniture and equipment. The
models presented were introduced by a set of information (Picture13). This regulation
influenced a generation of hospital architects, besides being an excellent source to study the topic
in Portuguese. We cannot leave unnoticed that many of its principles have endured
in the regulations to come.
Picture 13: Example of plans from the Ordinance 400/1977 (BRASIL, 1987, p. 92).
The Ordinance 400/1977 was an important
tool for educational purposes and to assure the quality of healthcare
facilities constructions until 1994, when the Ordinance1884/1994 (BRASIL, 1994)
was edited. The new Ordinance represented a radical change in the structure of
the regulations for healthcare infrastructure that had been previously
established.
To properly explain the context in which
the Ordinance 1884/1994 was conceived, we must understand the professional training
process established for architects and engineers by the Ministry of Health in
the 1980?s, after organizing the Specialization Courses concerning Architecture
in Health Systems (Cursos de Especialização de Arquitetura em Sistemas de
Saúde) in the University of Brasília (UnB).
Specialization Courses concerning Architecture in Health Systems
In 1981, the Ministry of Health, in
association with the University of Brasília (UnB), launched the first Specialization Course concerning
Architecture in Health Systems. Its primary goal was to train architects
and engineers from municipal and state health agencies to enable them to
design, approve and inspect projects and constructions of healthcare
facilities.
The content of this course, however,
went beyond studying the official regulations. At the time, there was a
Portuguese researcher at UnB, Professor Mário Júlio Krieger, who had just
gotten his doctorate in England, where he studied the principles of Architectural
Programming and its implementation in the English Healthcare System - still one
of the most highly regarded ones. Such principles, which used concepts from
topology, would be essential to write the regulations to come; many of the
architects graduated at that time took part in this movement.
Additionally, we must mention that by
getting financing for these courses from the Ministry of Health allowed UnB
resources to hire some of the most distinguished hospital architects at the
time to teach there, like Jarbas Karman and João Carlos Bross.
Among its students, we can list many
professionals who are still giving important contributions to the future of
architecture concerning healthcare in Brazil, like Flávio de Castro Bicalho and
Regina Maria Gonçalves Barcellos, who planned and organized the Ordinance
1884/1994; Mariluz Gomez Esteves, who helped organizing the Ordinance 1884/1994
and was chairman of the Brazilian Association for the Development of the
Hospital Building between 1998 and 2000; Frederico Flósculo Pinheiro Barreto, researcher
of Architectural Programming and Antonio Pedro Alves de Carvalho, who came to
organize seven editions of similar specialization courses in Salvador.
These courses, consequently, qualified
the future conceivers of the Ordinance 1884/1994, which was a forthright regulation,
functionally justified and with no strict demands concerning mandatory areas
and spaces.
Ordinance 1884/1994
The base for
Ordinance 1884/1994 (BRASIL, 1994) (Picture14) was the principles of
Architectural Programming, which basically means the study of the quantification,
relationships and dimensions of the spaces based on its functional
characteristics. Every room that appears in the regulation was thoroughly
studied for the activity to be held there, including the need for furniture, equipment,
people, further installation and inside/outside flows.
Picture 14: Cover of the book edition of Ordinance 1884/1994 (BRASIL, 1994).
To conceive it, not only the best
consultants in the area were gathered, as they applied an open methodology,
which allows easy updating and adaptation.
The architects Regina Maria Gonçalves
Barcellos, Flávio de Castro Bicalho and Maurício Freire Santiago Malta were
responsible for the general coordination and writing. As consultants, we may
list: Antônio Carlos Azevedo (doctor), Carmen Vieira de Sousa Unglert (doctor),
Domingos Marcos Flávio Fiorentini (architect and doctor), Eduardo Luiz Brito
Neves (engineer and administrator), Frederico Flósculo Pinheiro Barreto (architect),
Jarbas Karman (architect, administrator and engineering), Leni Helena Calixto
de S. Dias (doctor), Manoel Altivo da Luz Neto (architect), Maria Elaine
Kohlsdorf (architect), Maria Lúcia Ramalho Martins (nurse), Otto Toledo Ribas
(architect), Oviromar Flores (sociologist), Sandra Suzana Prade (nurse), Salim
Lamha Neto (engineer and administrator) and Tadeu Almeida de Oliveira (architect).
Dozens of other associates, from the most distinguished areas, have had a timely
participation.
There was no explanatory drawing in the
regulation, whose primarily goal was to develop a tool that would enable the
understanding that the activities to be held in a certain space, as well the
furniture and equipment necessary, would set the tone for the design of a
space. On that account, there were lists of activities linked to each room
specified in the overview table that identified the minimum areas and supplementary
conditions for the project. We can read in the introduction:
[...] it replaces the current regulation (Ordinance MS nº 400/77), which was rigorous and slightly flexible, and considers the physical planning of health systems.By adopting SUS's principles, including epidemiologic, environmental, cultural and geographic criteria, it replaces rigorous models for typologies that result from a collection of functional features when conceiving a building.Moreover, it deepens existing criteria and adds new ones, as a result we have alternative and varied solutions.[...] this document brings the technical foundation for conceiving and analyzing architectonic projects for healthcare facilities, being instrumental for the understanding of physical resources and for the quality of the healthcare service. (BRASIL, 1994, p. 6)
The first part of the regulation focuses
on how to present projects to the Health Surveillance Agency - such part now
belongs to the RDC 51/2011 (BRASIL, 2011b). The second part focuses on the Physical/Functional
Program, which says:
The methodology used to conceive the functional programs is listing, as extensively as possible, the collection of attributions and activities of healthcare facilities, which, in this text, we see as generic, not committed to any standardized solutions [...] (BRASIL, 1994, p. 28)
It discussed two itens:
- 1 - Attributions
- 2 - List of activities
For each attribution, there is a list of
activities that are related to the spaces of each Functional Unity. For
instance:
ATTRIBUTION #1: OFFER OF BASIC HEALTH SERVICES1.1-To undertake preventive healthcare services for individuals or group pf people, such as: immunization, first aid, control of communicable diseases, homecare, material collection for laboratory tests etc.;1.2-To undertake epidemiologic surveillance through: gathering and analyzing data, epidemiologic investigation, information about diseases etc.;1.3-To promote educational activities concerning health through lectures, demonstrations, in situ training, campaign etc. [...] (BRASIL, 1994, p. 32)
In chapter 3, there are tables by
Functional Unity, which are not just quantitative, but, mainly, establish
limits and conditions for the development of projects for healthcare buildings (Picture15).
Picture 15: Example
of a table from Ordinance 1884/1994 (BRASIL, 1994, p. 67).
The concept of Functional Unity is truly
important for the structure of the regulation. It means a collection of spaces
regarding complementing activities, instead of constructive typologies. For an
example: the spaces designed for first aid assistance must be consulted under
Functional Unit for Immediate Assistance, which is valid for either small
clinics or major hospitals.
There are some instructions to use the
tables that are worth the mention:
The existence of a certain space depends on the execution of its correspondent activity.Nonetheless, the execution of certain activity does not guarantee the existence of the specific space for it, since the activity may eventually take place in more than one space or with another activity in another space. (BRASIL, 1994, p. 43)
In Part III of the regulation, there are
additional information for healthcare facilities, such as: Indoors and outdoors
circulation; Environmental conditions regarding comfort; Environmental requirements
to control hospital infection; Ordinary and special building installations; and
Safety requirements to prevent fire.
Resolution from the Collegial Board 50/2002 (RDC-50/2002)
The RDC-50/2002 (BRASIL, 2004) might be
considered an update of the Ordinance 1884/1994, thus not presenting changes
concerning the methodologies for conceiving, presenting or advising. Only
updates and small additions are noticeable, resulting in a document in which
the Brazilian Health Surveillance Agency (Agência
Nacional de Vigilância Sanitária - ANVISA), created in 1999, takes on the
attributions to inspect healthcare facilities infrastructures (Picture16).
Picture 16: Cover of the RDC-50/2002 in its 2004 edition. (BRASIL, 2004)
In the presentation, it is stressed: "During
the updating process, the Ministry of Health has published several ordinances
on specific topics and the current work did not overlook the contents of those,
aiming at consolidating all the legislation there is on the topic." (BRASIL,
2004, p.3).
Such consolidation is the ideal path
towards better imparting and applying the regulations for healthcare
infrastructures.
There was an additional content that
must be emphasized: the detailed grounding of the used methodology in a text
with precise explanations of goals and reach of the regulations in item 3:
Dimensioning, Quantification and Building Installations of Spaces:
The current regulation does not establish a typology for healthcare buildings, like health centers, hospitals etc., here we attempted to regard all these buildings generically as healthcare facilities that must adjust to the epidemiologic, populational and geographic uniqueness of the region where they are sited. There are, therefore, different healthcare facilities, even when it is a building of the type of a health center, for instance.[...] by identifying in the list of attributions/activities from chapter 2 the number of the activity to be held, one must look for in the first column of each table the same number and thus the space correspondent to that activity.It is worth emphasizing that the space will only be mandatory if, obviously, the healthcare facility is going to hold the correspondent activity. [Italics added]Therefore, there are no pre-defined architectonic programs, yet, a list of spaces that must be used by the healthcare facility planning team as they are establishing the healthcare facility program or when the project is under assessment for approval.Each program is specific and must be conceived by the team planning the healthcare facility, including the needs and specificities of the project, therefore decentralizing decisions, which will no longer be made under a pre-defined foundation of programs or plans. (BRASIL, 2004, p.41)
Any attempt to modify the RDC-50/2002, as
a result, must take into consideration the methodology to do so and the use of
the regulation.
Regulations after the RDC-50/2002
Regulations from the Ministry of Health
are constantly being conceived by working groups. Several of them concern
infrastructure, complementing, revoking or adding new demands, ignoring the RDC
50/2002 methodology. Currently, there is no coordination that centralize those
changes, which are not only edited by ANVISA, but also by different agencies
inside the Ministry of Health.
It is very common to change the basic
regulations for projects and constructions of healthcare facilities, as we can
see in the RDC 36/2008 (BRASIL, 2008):
The physical infrastructure of the Obstetrics and Neonatal Unity must comply with the requirements from the Supplement II from this Regulation, which alter the items concerning obstetric and neonatal services from the RDC/Anvisa n. 50, from 21 February 2002. (BRASIL, 2008 [s.p.])
The Ordinance 11/2015 MS/GM (BRASIL, 2015), concerning
the Labor Unity, brings a table that only establishes minimum areas and
dimensions, with no reference to the activities held in each space. We may
observe that this table resembles the ones in the Ordinance 400/1977, i.e.
imposing quantities and areas not allowing adaptations to best suit each case.
In the RDC 07/2010 (BRASIL, 2010), concerning
the ICU, we read the following:
Section II: Physical InfrastructureArticle 10. The requirements established in the RDC/Anvisa n. 50, from 21 February 2002 must be followed.Sole Paragraph. The infrastructure must contribute to enable the privacy of patient, although not interfering with his or her monitoring.Article 11. The Adult, Pediatric and Neonatal ICUs must have their own and exclusive spaces.Paragraph 1. If these unities are contiguous, the support rooms can be shared.Paragraph 2. In hybrid Pediatric ICUs, there must be a physical separation between the Pediatric and the Neonatal ICU spaces. (BRASIL, 2010 [s.p.]).
It is noticeable that, although referring
to the RDC 50/2002, there are observations concerning infrastructure, which
makes the work for those involved in projecting and building a healthcare
facility very hard, since it implies a continuing study of all regulations, because
each one of them can have something concerning the physical area.
In the RDC 67/2007 (BRASIL, 2007), concerning
Compounding Pharmacies, there is no mention to the RDC 50/2002, establishing
demands for spaces that seem to be taken from a specific project:
4. PHYSICAL INFRASTRUCTURE.The pharmacy must be located, projected, built or adapted, with an infrastructure suitable to the activities to be developed, providing no less than:a) a space or room for administrative activities;b) a space or room for storage;c) a space or room for quality control;d) a space or room to weight raw material;e) room(s) to prepare the drugs;f) a space for distribution;g) locker room;h) changing room;i) toilettes;j) a place to clean utensils and packaging material;k) storage room for cleaning products. [...] (BRASIL, 2007 [s.p.])
There is no unity concerning the
structure or any other standard in the observations about the physical area
established in these regulations. The architects, engineers, administrators or
employees of Health Surveillance Agencies who work with healthcare facilities
projects must interpreted the details and goals of every regulation, since
reading cannot be considered a trivial task.
We must have a regulation for healthcare
facility infrastructures that comprehends all the observations on the topic and
that is constantly updated, preventing information from going astray, which
makes it impossible to fully understanding and applying it.
The Support System to Conceive Financing Health Projects (SomaSUS)
The SomaSUS project is of key importance to guide, impart and implement the
RDC 50/2002. It is an initiative from the Ministry of Health to compensate gap
in regulation concerning graphic information and architectonic programming.
The Executive Secretary from the Department of Health Economy,
Investments and Development from the Ministry of Health used to have difficulties
to guide architects and administrators through the projects presented that
needed approval for federal financing. The RDC 50/2002, although a
well-grounded regulation, fails to explain the essential information of
architectonic programming for the elaboration of projects, such as: indoor
flows, furniture, equipment, connection between activities and other regulations
concerning each functional unity. The graphic information to make some of these
data clear is lacking, especially for architects with no experience in the
field.
To compensate for this blank, the Ministry of Health, the Federal University
of Bahia (UFBA)/Studying Group in Hospital Architecture and Engineering
(GEA-hosp) and the Federal University of Santa Catarina (UFSC)/Institute of Biomedics
Engineering (IEB) teamed up to design an advisory guide for infrastructure
projects.
The UFBA was responsible for developing the graphic material for
architectonic guidance and the UFSC was responsible for equipment and
furniture, especially technical specifications and estimated costs.
The major issue faced at the beginning of this workforce was not to make
the same mistakes as in the Ordinance 400/1977 and before, which led to certain
architectonic solutions, by including complete plans of specific typologies. It
was decided that they would only explain the process of architectonic
programming established by the RDC 50/2002, which was based on the pre-dimension
of spaces, taking into consideration the activities developed, indoors and
outdoors flows, furniture, equipment and staff.
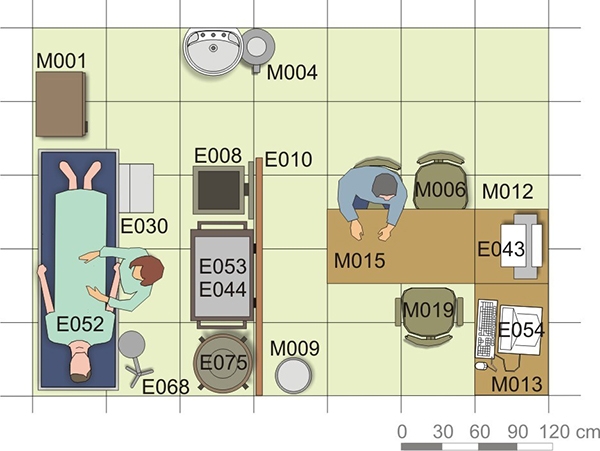
The result was modular plans, with no walls, divisions or miters, which
just explain the necessary spaces for each activity and suggested furniture and
equipment, thus not inducing pre-established solutions. Along with the graphic
schemes, there are tables that list furniture and equipment in the minimum
amount for each situation. To help the conception of financing projects,
they added estimated costs and technical specifications to that list. The didactic
and advisory style of the guide was, therefore, ensured since it was completely
based on the methodology used for the RDC 50/2002 (Picture 17).
Picture 17: Example of a layout presented in SomaSUS, with equipment and
furniture codes (BRASIL, 2017).
Initially, the work was made available through digital files recorded on
compact discs, which were distributed in meetings, seminars, congresses and to
the Health Surveillance Agencies. Later, the content was available on the
internet. In addition, a four-volume book was edited with part of that
content, to which case there were added scientific papers that better explain
how the studied functional unities work and that also include practical
examples with architectonic plans (Picture 18).
Picture 18: Cover of the volume 4 of SomaSUS (BRASIL, 2014)
SomaSUS is a valuable documentation for research and for professional
guidance for those working with healthcare infrastructures and that need a
material written in Portuguese and that is adapted to the Brazilian reality. This
is an important and enriching initiative concerning the technical aspects that affect
healthcare facility projects.
Further Initiatives
There are other initiatives of great importance that have been helping
to impart the knowledge related to healthcare infrastructure. The groundbreaker
was the establishment of the Instituto de
Pesquisas Hospitalares (IPH), by the architect Jarbas
Karman. The Institute have been carrying out an important work of
imparting and providing technical information concerning healthcare infrastructure
since the 1950's, by publishing books, magazines and launching graduation,
post-graduation and specialization courses (IPH, 2017).
Another important initiative are the Hospital Engineering and
Architecture Congresses that take place with the Hospital Equipment Fair (the Hospitalar), that happen every year in
the city of São Paulo. These congresses were initially organized by the Fundação São Camilo, which owns an
educational complex in administration of healthcare facilities. For many
years, those were the only permanent events to impart knowledge in the fields of
engineering and architecture concerning health (HOSPITALAR, 2017).
It is also worth mentioning the institution of the Brazilian Association
for the Development of the Hospital Building (Associação Brasileira para o Desenvolvimento do Edifício Hospitalar
- ABDEH) that, currently, has more than 600 members and is responsible for the
edition of books and magazines, in addition to organizing biannual congresses
that receive the presentation of scientific papers concerning healthcare
infrastructures at international level. The ABDEH's web page provides extensive
and free of charge material in this area of expertise for studying and
researching purposes(ABDEH, 2017).
The Studying Group in Hospital Architecture and Engineering (GEA-hosp), from
the Federal University of Bahia, Architecture Department, also has a relevant production concerning the topic. For instance, between 1997 and 2010, the
group organized specialization courses in architecture and health, having
published important books and, as it has already been said, took part in the
conception of SomaSUS (GEA-hosp, 2017).
Adding to the academic community, there is the work undertaken by the Espaço e Saúde group, an assembly of
professionals belonging to the Architecture post-graduation program from the
Federal University of Rio de Janeiro, which has also been organizing specialization
courses focused on architecture for health, as well as editing several books
and coordinating seminars (UFRJ, 2017). The Catholic University of
Brasília maintains, until nowadays, specialization courses to study
architecture and health (UCB, 2017). We cannot overlook the role of
several educational entities from the State of Rio Grande Sul, which coordinate
specialization courses of great importance that have been qualifying engineers
and architects to work with healthcare infrastructures since the 1990's.
The initiatives must be comprehended within the wide context of helping
regulating health infrastructures, since they represent highly qualified groups
that must interact in this mission of enhancing the quality of health
facilities.
Final Considerations
We are going through an important moment
of applying changes to the current basic regulation concerning healthcare
infrastructure. If there are properly grounded technical arguments, it will be
possible to continue with the discussions in a productive manner. However,
without this knowledge, the negative impact will be inevitable, reflecting in
the quality of the projects for healthcare facilities nationwide.
To accomplish a successful updating
process of the RDC-50/2002, we must seek:
- The maintenance (or deepening) of its methodology;
- The addition of changes that are present in later regulations;
- The development, within ANVISA, of a Coordinator Nucleus to manage the infrastructure regulations and that will centralize all the further modifications of the new regulation, making updating more frequent.
Therefore, it will be possible to
envision a process that points towards an evolution in regulation that keeps
the openness and informative style of the current RDC 50/2002. We observe that
the development of the legislation in health infrastructure must be accompanied
by the interaction with research institutions as well
as imparting and producing knowledge. This is a very specialized area,
therefore, it is necessary to continue the work of training and qualifying professionals,
as well as pursuing updates based on flexible premises and that are open to the
possibility of constant adequacy.
In the current process to update the RDC 50/2002, we must highlight the participation
of all these initiatives, which must be connected, to contribute effectively to
the technical training of the professionals involved.
Bibliography
ABDEH. Associação Brasileira para o Desenvolvimento do Edifício Hospitalar. Disponível em: http://www.abdeh.org.br. Acesso em: 21 abr. 2017.
BRASIL. Ministério da Saúde. SomaSUS: Sistema de Apoio à Elaboração de Projetos. Disponível em: www.saude.gov.br/somasus. Acesso em: 21 abr. 2017.
BRASIL. Ministério da Saúde. Portaria 11/2015 GM. Redefine as diretrizes para implantação e habilitação de Centro de Parto Normal. Disponível em: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2015/prt0011_07_01_2015.html. Acesso em: 21 abr. 2017.
BRASIL. Ministério da Saúde. Programação arquitetônica de unidades funcionais de saúde. V. 4. Apoio ao diagnóstico e à terapia: Anatomia Patológica, Hemoterapia e Hematologia, Medicina Nuclear e Patologia Clínica. Brasília, 2014.
BRASIL. Ministério da Saúde. Programação arquitetônica de unidades funcionais de saúde. V. 3. Internação e apoio ao diagnóstico e à terapia: Reabilitação. Brasília, 2013a.
BRASIL. Ministério da Saúde. Programação arquitetônica de unidades funcionais de saúde. V. 2. Apoio ao diagnóstico e à terapia: Imagenologia. Brasília, 2013b.
BRASIL. Ministério da Saúde. Programação arquitetônica de unidades funcionais de saúde. V. 1. Atendimento Ambulatorial e Atendimento Imediato. Brasília, 2011a.
BRASIL. Agência Nacional de Vigilância Sanitária. RDC 51/2011(b). Dispõe sobre os requisitos mínimos para a análise, avaliação e aprovação dos projetos físicos de estabelecimentos de saúde no Sistema Nacional de Vigilância Sanitária. Disponível em: http://www.paulinia.sp.gov.br/downloads/ss/resolucao_51_apresentacao_de_projetos.pdf. Acesso em: 21 abr. 2017.
BRASIL. Agência Nacional de Vigilância Sanitária. RDC 07/2010. Dispõe sobre os requisitos mínimos para funcionamento de Unidades de Terapia Intensiva e dá outras providências. Disponível em: http://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2010/res0007_24_02_2010.html. Acesso em: 21 abr. 2017.
BRASIL. Agência Nacional de Vigilância Sanitária. RDC 36/2008. Dispõe sobre Regulamento Técnico para Funcionamento dos Serviços de Atenção Obstétrica e Neonatal. Disponível em: http://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2008/res0036_03_06_2008_rep.html. Acesso em: 21 abr. 2017.
BRASIL. Agência Nacional de Vigilância Sanitária. RDC 67/2007. Dispõe sobre Boas Práticas de Manipulação de Preparações Magistrais e Oficinais para Uso Humano em farmácias. Disponível em: http://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2007/res0067_08_10_2007.html. Acesso em: 21 abr. 2017.
BRASIL. Agência Nacional de Vigilância Sanitária. RDC 50/2002. Normas para projetos físicos de estabelecimentos assistenciais de saúde. 2. ed. Brasília, 2004.
BRASIL. Ministério da Saúde. Secretaria de Assistência à Saúde. Manual de orientação para planejamento, programação e projetos físicos de estabelecimentos assistenciais de saúde. Brasília, 1994.
BRASIL. Ministério da Saúde. Secretaria Nacional de Organização e Desenvolvimento de Serviços de Saúde. Normas e padrões de construções e instalações de serviços de saúde, 2a ed. Brasília, 1987.
BRASIL. Ministério da Saúde. Secretaria Nacional de Ações Básicas de Saúde. Normas e padrões de construções e instalações de serviços de saúde. Brasília, 1979.
BRASIL. Ministério da Saúde. Secretaria de Assistência Médica. Normas do Hospital Geral. Brasília, 1974.
BRASIL. Ministério da Saúde. Departamento Nacional de Saúde. Projeto de Normas Disciplinadoras das Construções Hospitalares, de Oscar Valdetaro, Roberto Nadalutti. Rio de Janeiro, 1965.
BRASIL. Ministério da Saúde. Serviço Especial de Saúde Pública (SESP). Padrões Mínimos Hospitais, de Oscar Valdetaro, Roberto Nadalutti, Israel B. Correa e Hélio Muller, 194?. Fonte: acervo IPH.
GEA-hosp. Grupo de Estudos em Arquitetura e Engenharia Hospitalar. Disponível em: https://geahosp.wordpress.com. Acesso em: 21 abr. 2017.
HOSPITALAR. Feira+Forum Hospitalar. Disponível em: http://www.hospitalar.com. Acesso em: 21 abr. 2017.
IAB. Instituto de Arquitetos do Brasil. Departamento de São Paulo. Planejamento de Hospitais. São Paulo, 1954.
IPH. Instituto de Pesquisas Hospitalares Arquiteto Jarbas Karman. Disponível em: http://www.iph.org.br. Acesso em: 21 abr. 2017.
RENOVATO, Rogério D.; BAGNATO, Maria Helena S. O serviço especial de saúde pública e suas ações de educação sanitária nas escolas primárias (1942-1960).Educar em Revista, Curitiba, Brasil, n. especial 2, p. 277-290, 2010. Editora UFPR.
UCB. Universidade Católica de Brasília. Curso de Arquitetura de Sistemas de Saúde. Disponível em: http://www.ucb.br/Cursos/185ArquiteturaDeSistemasDeSaude. Acesso em: 21 abr. 2017.
UFRJ. Universidade Federal do Rio de Janeiro. Grupo de Pesquisa Espaço Saúde/PROARQ. Disponível em: http://www.proarq.fau.ufrj.br/novo/pesquisa/grupos-de-pesquisa/18. Acesso em: 21 abr. 2017.
USA. United States of America. U.S. Public Health Service. Elements of the General Hospital, 1946. Disponível em: https://babel.hathitrust.org/cgi/pt?id=mdp.39015029959809;view=1up;seq=3. Acesso em: 09 abr. 2017.
Share




Send by e-mail: