Publications IPH Magazine IPH Magazine #16 "Casinha": The story of the Birth Center in Rio de Janeiro that became a model for humanized labor and resistance to the hardships of public management

- An analysis of the sectorization and comfort in contemporary children's hospitals
- "Casinha": The story of the Birth Center in Rio de Janeiro that became a model for humanized labor and resistance to the hardships of public management
- Risk of infections caused by the presence of the fungus Aspergillus.sp: remodeling hospitals and climatization systems
- Health financing systems worldwide
- A pathway for death: the flow and connections between environments and its occupants
"Casinha": The story of the Birth Center in Rio de Janeiro that became a model for humanized labor and resistance to the hardships of public management
Cristiane N. Silva

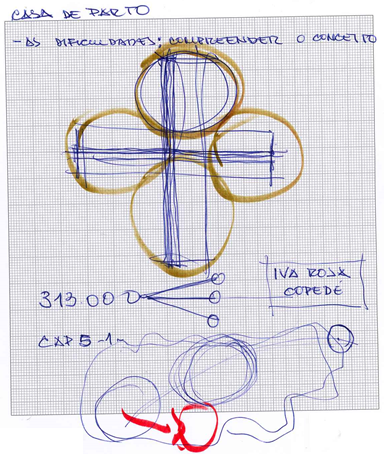
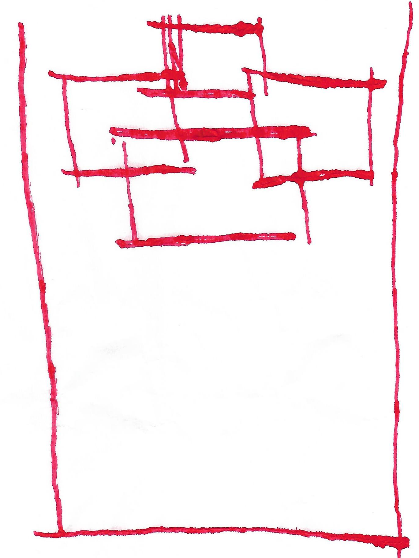
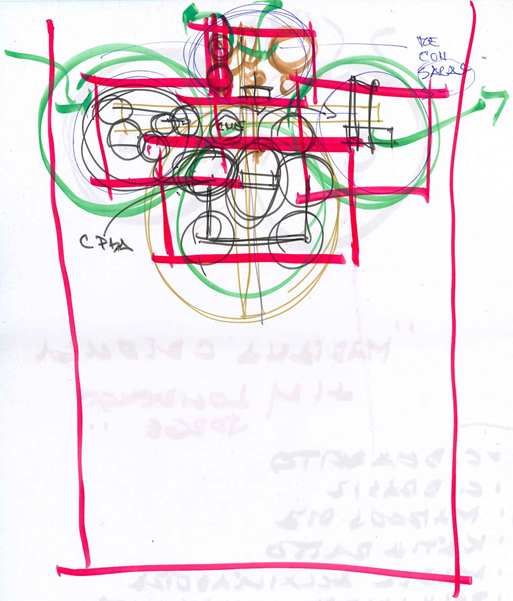
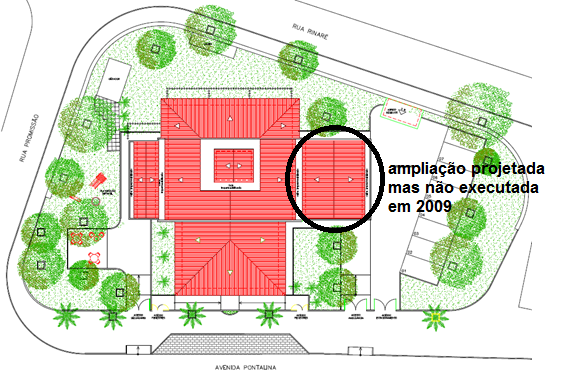



Photo credit: Adriana Medeiros (2018)
Introduction
This article is part of the thesis presented by the author to PROARQ / FAU / UFRJ to obtain the PhD in Architecture [1]. The thesis investigates the environment in birth centers, with specific focus on normal delivery centers, observing the sensitive aspects that impact and influence the perception and subjectivity of the users in such environments. The author used qualitative and quantitative research methodologies in two case studies, both in normal delivery centers in the city of Rio de Janeiro. One of them, the David Capistrano Filho Birth Center, is presented as a model due to its role in the movement to humanize childbirth and in this city and the results found during its evaluation as part of the case study. "Birthplaces" (BITENCOURT, 2007), within the structure of healthcare facilities, can be regarded as places where patients go to not looking for a diagnosis - after all, as the popular saying goes: "pregnancy is not a disease" - but mainly assistance, care and attention to safely birth their children. In contrast to the inherent negative feelings usually triggered inside the hospital environment, such as fear and vulnerability, they are positively associated with the arrival of life, or should be, since this is not the reality found in most public institutions intended for childbirth in Rio de Janeiro.
The spaces intended for labor and birth, in their formal and physical configuration established for Birth Centers inside hospitals, cannot meet the needs of users with regard to providing environments that invoke privacy, identity, appropriation, safety and control, among others that guide and change the experiences and personal impressions each woman has of such environments. It is precisely in this context that David Capistrano Filho Birth House - or "Casinha" - stands out, for achieving results that prove it can be an excellent example of how to plan, design, build and care for a "birth environment". One that satisfies nearly every expectation concerning the environment and makes clear the need for elements that go beyond the physical composition, involving resources, planning, differentiated work methodology, empathy, team training, education and information, among others that, together and in an appropriate physical structure, lead to very positive experiences for those who experience such work, enjoy the interaction, the power of being in charge and the positive experience of childbirth for women and their families.
1. Birthplaces: in search for the human dimension
The institutionalization of humanized care for women, advocated by the Ministry of Health, aims to guarantee pregnant women access to decent and high-quality care during pregnancy, labor and puerperium. (BRAZIL, 2000) The humanization of childbirth movement in Brazil was encouraged by experiences that have been carried out throughout various states since the 1970s as well as by professionals inspired by practices used by former midwives or even the indigenous tribes of the country. In the 1980s we saw the creation of many groups that not only offered humanized care for pregnancy and childbirth, but also proposed changes for such practices. These movements support, promote and demand humanized childbirth care in all its stages, beginning at empowering women and emphasizing the mother/baby unit and evidence-based medicine. Among their goals, we can enlist: the end of medical interventions used just at the convenience of one or both parties (physician and patient) or the hospital; the respect for each woman's particularities and preferences for the moment of her labor; the redefinition of human relations in healthcare; the understanding of labor as a sacred moment and therefore deserving of reverence (DINIZ, 2005).
Regarding architecture, the humanization of childbirth brings two fundamental aspects: the first is establishing that healthcare facilities are accountable for receiving with dignity the woman, her family members and the newborn, which requires, besides changing the care provided by doctors and other health professionals, an intervention in the physical organization, in order to create a receptive and welcoming environment. The second item foresees the adoption of measures and procedures known to be beneficial for monitoring the labor and birth (DINIZ, 2005), which includes thinking about the spaces intended for childbirth. When considering the role of architecture, it is up to this area of expertise to find ways to give back to childbirth the familiar, welcoming and familiar environment that medicalization disrupted and transformed into the cold, controlled hospital environment that can be perceived as an "impersonal and unknown" place, giving rise to situations that range from discomfort and coldness (COELHO, 2003) to loneliness and depression.
The architecture projects for labor and childbirth have been reviewed and reappraised over the past decades, along with other issues related to obstetric care practices in Brazil, with great encouragement of institutional programs, through standard rules, manuals and specific guidebooks that outline proposals for the qualification and humanization of the physical structure in the spaces of birth.
1.1. Birth Centers
Labor is influenced by a series of physical and emotional issues that interfere with women's feelings, involving psychological, physical, social, economic and cultural aspects. Providing an environment for childbirth that can provide parturient with the possibility of appropriation and control might also minimize the strangeness and insecurity that come from being in an unfamiliar environment that leads to illness and the fear of giving birth due to other experiences she lived or was told; and even on issues related to family culture and customs. This is precisely what the concept of ambience suggests when it establishes the relationship between the individual and the environment, observing it from a perspective guided through every relevant personal aspect: feelings, knowledge, culture, expectations, fears. The subjective effects that rise from this range of sensations act on and with the perception of the environment, causing the sensitive experience lived by the subjects exposed to it.
The concept of woman-and-baby-focused care during labor has broaden, and these changes in behavior and being in charge have altered the way maternity services are thought and organized. Still, even with the many rules and recommendations in place, few changes have actually been made. When designing environments for labor, the need for security, comfort and privacy that all women have at such unique moment must be considered. It should also be considered that these sensations, as well as being satisfied or not after such an experience, are directly influenced, among other factors, by the environment where labor/childbirth took place, which could be either traumatic or satisfactory. (WALSH, 2007)
When designing environments for labor, one should consider the necessity to provide women with a sense of freedom to come and go, so they feel safe and assured, and have the right to be with their friends and family, if they wish to, providing privacy and personal control, so women can feel safe, relaxed, comfortable and in charge of their labor. These are the concepts that underlie the recommendations, norms and philosophy of the projects intended for natural birth centers[2] (SILVA, 2018b).
The strategy to implement Birth Centers in Brazil began in the late 1990s, gaining priority with the creation of "Rede Cegonha" in 2011 and becoming one of the main strategies in the context of the propositions of an innovative obstetric model for labor and childbirth (DE VICO, 2017). The Birth Centers are healthcare facilities for labors that present the usual risk and that belong to or are associate with a hospital, being located inside or outside the institution. They are independent from the obstetric operating room, they carry out humanized care, exclusive normal delivery without dystocia[3] and privilege women's privacy, dignity and autonomy by enabling them to give birth in a more welcoming and comfortable environment, where they can have be with whoever they choose to be.
Birth Centers are facilities planned and equipped with elements to enable women to go through an active and participatory labor, using practices that set them apart from the traditional obstetric care of the last decades and following the World Health Organization recommendations 1996 ( AX AND SQUARE, 2006). The Birth Centers were created with the goal of "giving pregnant woman the opportunity to exert their rights regarding privacy and dignity" (MACHADO E PRAÇA, 2006), allowing her to give birth under conditions similar to those she would find at home without, however, giving up access to technological resources in case of any complications during labor.
The healthcare model found at Birth Centers minimizes the hierarchization in patient/health professional relationship, includes the family in the childbirth process, granting the mother-to-be the right to have someone by her side throughout the process, and aims at making the moment of childbirth as pleasant and safe as possible (SILVA, 2015). To meet such needs, the physical space intended for childbirth had to undergo changes, investing the architect plan of Birth Centers with fundamental importance to fulfill the role and goals of healthcare facilities. It is necessary for the architect to scale, during the design process, the implications of the relationship between the environment and its users, as well as the issues related to humanization and ergonomics.
1.1.1. Relationship with the attributes of the environment: Design and practice
There are numerous issues that interfere with women's feelings during labor, which may even influence its progress and conditions, issues that involve the physical and emotional aspects of childbirth itself, but may also include psychological, physical, social, economic and cultural aspects. Considering such issues from the perspective of projects for environments intended for childbirth, even more so if dealing with Birth Centers, it becomes more important to ascertain which physical elements of these environments can be related to the attributes of ambiences when trying to qualify the project and the environment for childbirth.
The set of feelings aroused by the material and immaterial elements, which identify the way each one perceives the spaces, characterizes the ambience of each one of them. The ambience expresses the material and moral atmospheres that permeate and involve sensations related, for example, to light, sound and temperature of the environment (AMPHOUX, 2004 quoted in SILVA, 2018b), as well as sensations related to privacy, identity, control, security, territoriality, among others. Ambience studies do not simply consider the composition of space, but its interrelationship with the sensitive experience that is brought about by the people who inhabit it (SILVA, 2018a). For this study, the author observed attributes concerning the following items:
- Reception and welcoming (front desk): The front desk is the first place where the woman and her family should feel welcomed upon arriving at the maternity clinic. It is the gateway to the place that is intended to provide the mother with confidence, help and a sense of welcome, where she can begin to feel safe from the beginning of her birth process. It is also where sheltering starts and, therefore, it is of paramount importance that the process of humanization and qualification of the environment begins there too. The proper reception of women and their caregivers, considering all these aspects, contributes to the establishment of a bond of trust and security, helping in the tranquility of the pregnant woman and her role in labor.
- Normal Labor Room: One of the main spaces that characterize a Birth Center is precisely the Normal Labor Room, intended for carrying out pre-labor, labor and after labor procedures. The ruling RDC 36/2008 describes them as "a unique and reserved environment for monitoring and conducting labor, delivery and observation of women and their newborn in the first hour of life". Bringing together all the procedures related to the stages of childbirth in one environment is intended to prevent the transfer of women in labor from one environment to another, and to provide women, their babies and their caregivers with a quiet and reserved place also in the period after childbirth, even if during the minimum period established. In Birth Centers, women stay in the rooms since pre-labor until mother and baby are discharged. These rooms, in general, are designed to recreate a residential, familiar and completely different configuration from the traditional operating rooms, giving the patient feelings of comfort, well-being and confidence. These are places where women can experience childbirth assisted by familiar caregivers or friends who can provide ongoing care. Women receive help to become confident and optimistic in private, sacred and safe spaces (WALSH, 2007).
- Aspects related to culture and the issue of companions: It is necessary to observe other aspects related to birth spaces that can generate different perceptions of the environment according to the cultural aspects that involve the individuals, since, from a symbolic point of view, the environment and its components are related to the cultural and social codes that are human. People live, not only incorporating, but also reproducing countless meanings related to the architecture spaces and their functions (SILVA, 2018 a). In this regard, it is essential to consider not only the mother and the baby, but also those chosen by her to be by her side during that period of personal, family and social transition represented by the birth and the arrival of this new person to the interaction of all.
Even considering pregnancy and childbirth as normal and physiological aspects of a woman's life, each one experiences it as a special and different moment, with unique experiences that include sudden physical, emotional, social and family changes, shared with family, friends and groups to which she belongs. Allowing her the freedom to choose whoever she wants to be by her side during reception, labor, childbirth and immediate after childbirth, besides being her right, is also one of the prerogatives directly related to the fulfillment of these desired conditions of comfort, tranquility and safety in the process of labor and childbirth. Even with laws and countless researches that indicate the benefits of having someone with the woman during childbirth, the percentage of pregnant women who go through this moment without someone of their choice, either for not knowing their rights or for being forced by the healthcare team, in public and private healthcare facilities, still reaches significant levels (FERREIRA AND MADEIRA, 2016; RODRIGUEZ ET AL, 2017).
The presence of a companion during the birth process is a practice that favors safety, quality of care and humanization of care; besides incorporating and being in compliance with SUS (Brazilian National Health System) policies on integrality, universality and equity in women's health care. It can be expected from its complete implementation positive changes: for women, increased sense of security and support, respect, comfort and bonding with their family and social network; for the staff, an encouragement to change the paradigms regarding the established obstetric practices and to embrace new ways of thinking about care and health management practices (PEACE and FENSTERSEIFER, 2011; DINIZ ET AL, 2014).
2. David Capistrano Filho Birth Center, also known as "Casinha"
David Capistrano Filho Birth Center opened on March 08, 2004 by the Rio de Janeiro Municipal Health Department. It is established in Realengo neighborhood, on the west. The Birth Center or "Casinha", as it is called by its users, has 374.50 m² of built area and is located in an extremely vulnerable area of the city that lacks basic assistance resources. Still, it is of fundamental importance as a reference for prenatal care and natural childbirth in this region and the surrounding area (AZEVEDO, 2008).
Illustration 1 - David Capistrano Filho Birth Center/RJ
Photo credit: Adriana Medeiros (2018)
2.1. Implementation
The implementation of this Birth Center, the only one of its kind in the city until the present day, is a direct result of discussions about the medicalization of childbirth and the excess of interventions that it underwent, which increased in Brazil in the eighties with the promotion of forums for discussion that mobilized society, professionals and the academic environment involved in questions about the qualification of obstetric care in the country. These debates and movements have encouraged various governmental actions in the search for the humanization of childbirth, such as the insertion of obstetric nurses in labors, qualification of this professional category, the limitation of the number of cesarean sections performed through SUS (PEREIRA ET AL., 2012), as well as the concern with the qualification of the space destined for labor and birth.
Even with the motivation to qualify and humanize childbirth, having obstetric nurses inside municipal childbirth centers repeats the historical questioning about the qualification and the need for "medical knowledge" to the detriment of nurse knowledge and performance to conduct and assist women throughout the process. Besides the professional competence of obstetric nurses, they call into question practices regarding the humanization of care, such as ambulation, the use of balls, waterbirth, the use of other birthing positions, besides the traditional lying down, the restriction of episiotomy[4] and other unnecessary interventions (PEREIRA ET AL., 2012). In this context of actions and discussions on actions for the humanization of childbirth, SUS Birth Centers were also established in the country through the Ordinance / GM No. 985/1999, enabling their implementation in municipal health systems.
Even if officially established by this first Ordinance of the Ministry of Health as an ideal healthcare facility aimed at carrying out normal births, the establishment of the Birth Center in Rio de Janeiro had neither a quick nor an easy story. The initiative of the Municipal Health Secretariat - SMS / RJ came after the opening of Sapopemba Birth Center (SP), by David Capistrano[5] who, in 1999, coordinated the regulation and implementation of this type of health unit within the SUS. The David Capistrano Birth Center is the third of its kind in the country before the creation of any regulation for it.
David Capistrano Filho Birth Center, opened on March 8, 2004, has been through countless conflicts resulting from disputes between the favorable and unfavorable segments of this type of assistance, even involving actions in the Public Prosecution Service (PEREIRA ET AL., 2012). They ranged from lawsuits filed by CREMERJ (Rio de Janeiro Regional Medical Council), with questions about the "illegality of services" due to the absence of doctors in the service (PEREIRA E MOURA, 2009), and prohibitions by the State Health Surveillance for lack of a license that the regulatory agency itself had not issued because it did not recognize the new health facility model.
Through each one of these hurdles, it was crucial to rely on the great mobilization of entities that advocate for humanized childbirth and women's right to choose the place and the most appropriate form to have their children, if there are no complications. This mobilization eventually prevailed, and the Sanitary Surveillance Superintendence granted the Birth Center the right to operate in November 2009 (PEREIRA et al., 2012).
2.2. Project and implementation:
An initial difficulty faced in the conception of the Birth Center concerned the distribution of spaces, since there were no established guidelines for the design of this new typology of environment for childbirth. The main direction that guided the project for Rio de Janeiro's Birth Center was the search for domesticity, that is, references that refer to the safe space of the home. And the result was a Birth Center that did not have "the mirror of the hospital delivery unit under any circumstances" (BITENCOURT AND COSTEIRA, 2018). In addition to the issues regarding the need to develop a new model for the facility intended for normal birth in the city, there was also great pressure against the implementation of this new model.
Architect Iva Rosa Copedé, from SMS / RJ, was responsible for the project with the guidance and collaboration from Fábio Bitencourt. Their starting point was a symbol used to represent both SUS and healthcare: a cross (Illustration 2). From this cross, wards were created and from these, the ideas of how to house the assistance to be provided would be defined. According to Fábio Bitencourt, the conception started from an initial drawing around this cross, where wings were created (Illustration 3). From this conformation, a large area for effective assistance was created, which would be exactly the largest space (Illustration 4). The main areas that would be the basis of the building were then defined (Illustration 5) and would be subdivided into different environments (Illustration 6). Subsequently, this idea of sectorization was taking shape (Illustration 7) and combined in the final idea (Illustration 8) for the first draft of the architecture that would be developed for the birth center (BITENCOURT E COSTEIRA, 2018).
Illustration 2 - First items intended for the elaboration of the concept of Rio de Janeiro's Birth Center: architecture concept, financial availability and location.
Source: Fabio Bitencourt's drawing (2018)
Still, there was a long way to go to find out what the necessary environments would be and how to adapt them to the current generic norms for the design of healthcare facilities intended for childbirth respecting the lines proposed by obstetric nurse professionals and by the architects involved in the project. There were still work processes and environments to be defined, such as the Normal Labor Room, which had already been named, but that was still a tricky issue architects had to solve in the project.
Professionals specialized in women's health were interested and tried to assist in the processes, since it was an idea still in progress for everyone. There was no architecture guideline established as there is today. The first legislation with ruling close to the current standards, the RDC 36, would not come into force until 2008, almost a decade later. Therefore, each part of the birth center was conceived as a novelty, designed according to the activities that were emerging and the needs that were gradually being guessed by the professionals involved in the conception.
Illustrations 3 to 7 - Initial Conceptual Planning Process for the Birth Center
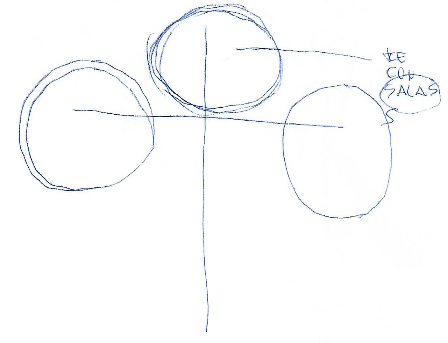 Illustration 3
|
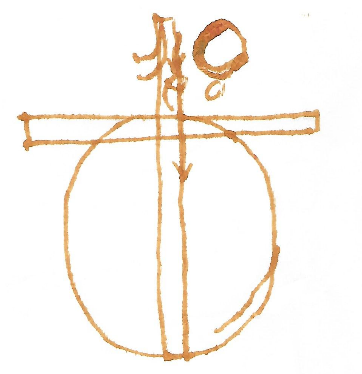 Illustration 4
|
 Illustration 5
|
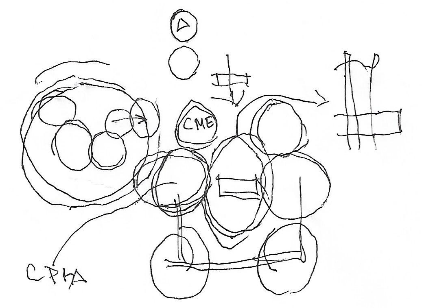 Illustration 6
|
Illustration 7
Source: Adapted from Fabio Bitencourt's drawing (2018)
The environments were designed and created from the main entrance: there should be rooms for mother's activities, a breastfeeding plan, a plan for women who had already been through a normal birth; toilets; a room where parties and meetings could be held, considering the large outdoor space; a reception; a gynecology office with attached bathroom and a room for the administration of the house. The two "modules besides the cross" would concentrate services and logistical support on one side; on the other side, there would be an area to enter and exit the center, as well as an access to the ambulance on duty. In the service area, a purge area, a home-like laundry room, and a kitchen. Between the reception and the internal area there would be a balcony, a reception that would make the transition to the interior space, where there would be a nursing station, another room, which would be intended for curettage, gynecological procedures, attention and evaluation of women. In addition, four rooms for normal labor were also designed. One of them was later transformed into a rest area for the nurses. In the central area, a nursing station / prescription area would be located.
Each one of these environments, as well as their interconnections, moves towards an architecture design defined as two great intersecting axes and are complimented until they become the blocks conceived by the architects: the central blocks, which receive the effective assistance (the rooms, the front desk, the nursing station and the prescription area); the side blocks, which serve the service area and the alternative entrance and exit for patients and ambulance personnel; and the front area, intended for front desk, welcoming, events, meetings and administration. It is according to the distribution of these uses and the processes inserted in them that the architecture takes shape, adapting to the size of the land available for implementation.
The final composition of the project is a very simple structure, complete with an office, a meeting room for educational groups (still called a utility room), a waiting room, a nursing station, a delivery room or a care room that could function as office, three admission suites, board room, laundry room, storage room for consumables and kitchen and solarium in the central area. Outside, there were the parking lot and the patio. The house received "a soft-toned ambiance, wicker furniture, colorful pillows, pictures of women and children in activities in the unit itself, making the environment very welcoming" (AZEVEDO, 2008).
Illustration 8 - Final draw of the conceptual planning for the Birth Center
Source: Fabio Bitencourt's drawing (2018)
Illustration 09 - Implementation - David Capistrano Filho Birth Center - Renovation Project - 2009
Source: SMSDC / RJ
Illustration 10 - David Capistrano Filho Birth Center's current layout
Source: Cristiane N. Silva as-built, 2018.
In addition to the physical and structural configuration of the building, the "atmosphere of domesticity" initially sought and that guided the architecture program for the Birth Center is intensified by the planned and installed ambience, with pink and salmon interior and exterior painting; furnishings reminiscent of a homey atmosphere starting at the front desk all the way to the labor rooms, including armchairs, pillows, double beds, among other objects that can be found in any residence; creating recognizable and welcoming environments for the "clients", their families and everyone else who occupy the center. These characteristics remain virtually unchanged to the present day, after fifteen years of operation. Even though the current need of the Center to receive care is noticeable, such as repainting; correction of capillary infiltrations common in surrounding areas; lawn mowing and various repairs to the physical structure, which catches the eye as soon as you enter the reception area is the atmosphere of the place, which welcomes, nurses and makes all visitors feel at home.
2.3. Reference Assistance Facility
Since this is a Birth Center independent from any hospital facility, it relies on Mariska Ribeiro Women's Hospital, in Bangu neighborhood, as a reference center in case of emergencies. The referral hospital is roughly five kilometers away from the Birth Center, a distance traveled by ambulance, with the siren on, within approximately ten to fifteen minutes during the worst rush hour.
This Birth Center offers mothers prenatal care during all stages of pregnancy, achieving as main results not only a better monitoring of the pregnant woman's condition, aiming at the normal delivery, but also the "prior knowledge of the mother and her family, her social, emotional and biological situation, the possibility of bonding with the professionals and the unit" (AZEVEDO, 2008).
The Birth Center principles are: offering "a safe and pleasant space for women and families who wish for (...) a natural childbirth with a minimum of interventions, active participation of women, the right to listen, verbal and bodily manifestations", besides deconstructing the current medicalized model of childbirth, in return to a physiological and feminine moment, in an "emancipating, polemic and counter hegemonic" model (CPDCF, 2018).
Due to its characteristics and background, the Birth Center receives only minimum-risk pregnant women, serving not only the women in their area of coverage, but all of those who fall outside the limits imposed for the safety of women and their babies. Until 2019, the Birth Center have delivered 3,260 babies with no maternal mortality and only two cases of complications with newborn infants who were referred to and assisted at the referral hospital.
3. David Capistrano Filho Birth Center - User Assessment
The research that inspired this article was based on the evaluation of aspects of the ambience found at birth centers analyzed in order to verify possibilities of detecting factors that could effectively interfere and influence the perception and experience of these environments by their users. The comparative table (Table 1) shows the association between the attributes of the environment considered in the forms of the qualitative tool - Aspect - in the booklet of the Institutional Environment and the attributes considered by the researcher for the study:
Table 1 - Index of items listed in forms x Ambience Manual x attributes considered for the research.
Source: Cristiane N. Silva
Table 2 presents the individual grades assigned to each of the items in Aspect tool assessment forms, according to the opinion of each participant about the Birth Center.
Source: Cristiane N. Silva
Most of aspects assessed received similar grades/evaluations from almost all respondents. Overall, the ratings are positive. The results were also evaluated, by way of verification, by the standard deviation calculation, with very similar results. The items assessed were as followed:
- Privacy, companionship and dignity: Patients, caregivers, and staff acknowledge that this is fully fulfilled by the physical facilities designed for the Birth Center. This item is directly related to the comfort conditions, focusing on the privacy and individuality of users. Questions regarding the delimitation of personal space, control and privacy are directly answered by the existence and use of the Normal Labor Rooms. These environments allow "clients" the opportunity to obtain an individualized and comfortable space, equipped with appliances designed to give women the choice and control over almost every aspect of their labor process and stay. The Normal Labor Room, as used in the Birth Center, also provides the choice of whether or not to relate to people outside the family circle and friends, which does not exist in a shared ward, and primarily the relationship between the family and the newborn member.
Illustration 11 - Patients, caregivers and professionals - Delivery and post-childbirth in the Normal Labor Room.
 |
 |
Photo credit: Adriana Medeiros (2018)
Also regarding control, a primary aspect to be mentioned is that, whenever possible, all the determinations and desires established by the woman in her birth plan[6] are followed at will, as long as they do not imply risk to the mother or the baby. The issues of appropriation, identity and territoriality permeate the use of Normal Labor Rooms, but are also greatly influenced by the homely atmosphere and the general appearance of the Birth Center, which refer directly to recognizable and welcoming environments, offering a sense of security completely different from the ones we have contact with in an environment with imminently hospital characteristics.
These issues are also directly linked to the empathy bonds created during prenatal care, through group meetings aimed at clarifying issues related to pregnancy, childbirth and baby care, in which pregnant women participate. These meetings also contribute to the knowledge and recognition among professionals, patients, family and the environment of the Birth Center, establishing bonds and appropriation, giving meaning to the spaces and making them a "place" for all its visitors, who affectionately call it "Casinha".
The last two items considered, environmental perception and culture, permeate all the others and, in relation to the Birthing Center, are influenced by them, giving the others the same influence. Environmental perception is influenced not only by the physical and compositional aspects of environments - such as shape, colors, furniture typology, the use of walls as murals to express clients' expectations - but also by guidelines on women's rights and the smell of a cake baking in the kitchen that is felt all the way through the front desk.
Illustration 12 - Group meetings and bonding - Birth Center
 |
 |
Everything at the Birth Center welcomes you. Such welcoming, combined with the feeling of having privacy and control, having personal references, being surrounded by the people of your choice, and the differentiated care treatment, are fundamental, according to the testimony of some patients, to bring the feeling of security and comfort regarding the childbirth, minimizing the fears and concerns brought about from other women's stories or past experiences.
Illustration 13 - Welcoming, atmosphere, ambience - Birth Center
 |
 |
 |
 |
Photo credit: Adriana Medeiros (2018)
- Outside view: Patients, caregivers and staff agree that this is fully fulfilled by the Birth Center. The Birth Center offers clients and staff ample access to the outdoor landscape through the windows in the rooms and offices, as well as the doors that are always open to the gardens, even if they lack the necessary maintenance. Natural light is also present, passing through windows, open doors, glass bricks and skylights. The circulation outdoors is unrestrainable, further facilitating access to these areas.
Illustration 14 - Outside view and natural light
 |
 |
Photo credit: Cristiane N. Silva (2018)
-
Nature and open air: Patients, caregivers and staff agree that this is fully fulfilled by the Birth Center. This item interferes with aspects related to environmental control and perception. Control is given precisely by the possibility of unrestricted circulation and access to all environments, allowing customers and employees to look at environments where they stay for several hours at a time, if they wish.
Despite the expressive evaluation, it is worth consider that although the possibility to access and contemplate the outdoor area, it is little visited and noticed, especially by customers, who generally prefer to stay in the rooms. That can be mainly caused by: the extreme heat, common in the neighborhood; the lack of a better maintenance of the gardens; the lack of equipment that could provide comfort and protection to customers would enjoy the outdoor space, both against the sun and the sight of those who pass on the streets surrounding the Birth Center.
Illustration 15 - Outdoor area - Gardens - Birth Center
 |
 |
Photo credit: Cristiane N. Silva (2018)
- Comfort and Control: Patients, caregivers and staff agree that this is fully fulfilled by the Birth Center. The possibility of being in a private space during admission is a crucial item regarding the clients' appropriation over their personal space, enabling actions that would be impossible in shared wards and acting in the appropriation of the space and the maintenance of the identity. Families can bring personal items to display and use during their stay and have alternatives to regulate the incidence of lighting. One of the main items about the feeling of comfort and control provided to women refers to the possibility of giving birth the way they wanted, in a familiar environment and with personal references, using the method and position they chose, whenever possible.
- The legibility of the center: Patients, caregivers and staff agree that this is fully fulfilled by the Birth Center. This item mainly relates to environmental control and perception, both referring mainly to the possibility of decision-making and the security of the environment in which individuals find themselves, how they can act, transit, enter or leave, locate themselves and obtain information on procedures, processes and essential rights for the typology of care performed there. The possibility of legibility of the place also brings with it a sense of security, arising from the knowledge and appropriation of spaces.
Illustration 16 - Outdoor area - Access and surrounding
 |
 |
Photo credit: Cristiane N. Silva (2018)
- Inside aspect: Patients, caregivers and staff agree that this is fully fulfilled by the Birth Center. It relates mainly to personal space, appropriation and identity, environmental perception and culture. As this is an aspect whose interpretation is most profoundly influenced by personal taste, experience, history, and preferences, it could have received more divergent assessments, nonetheless, with rare exceptions, it received a score below five points, even considering the obvious needs of maintenance perceived in almost every room. Although the problems regarding the visual aspect are visible and perceived by customers, visitors, and employees, they lose weight and importance in light of all the work done there and the results achieved.
Illustration 17 - Inside aspect - Ambience
 |
 |
 |
 |
Photo credit: Cristiane N. Silva (2018)
The items related to the indoor aspect mention spaces that refer to home and recognizable environments, which is perfectly found in the Birth Center. These environments are kept extremely clean, the ceiling fans help drift temperatures in areas without air conditioning. Open doors and windows give the feeling of lightness and airiness. The existing floor, wall and ceiling coverings are not uncommon, they are the same since the inauguration and are repeated by the environments, from the pink of the walls to the ceramic tiles of the floors. There is no variety or luxury, but there is a kaleidoscope of posters, paintings with messages from previous patients, pictures with people important to the Center, the various awards received, indoor garden with plastic flowers, chairs of different materials, picture frames on tables and walls. Mobiles crafted by the nurses for some party hanging from the ceiling. There is no shortage of the diversity of cladding materials or the paint color of the walls. The indoor aspect of the Birth Center is at once all alike and completely different. It has its own identity, it is welcoming and pleases its admirers, who would like to see more attention towards preservation, but fully identify with the environments, help with its ambience and completely own that place.
- Facilities: Patients, caregivers and staff recognize that, even though the Birth Center fulfills this aspect satisfactorily, there is still some need for improvement. This item covers the general amenities offered to customers and the safety and comfort conditions found in the environments, especially in the bathrooms inside Normal Labor Rooms. Most of the items listed received good grades, and we can say that the grade proportionally lower than the other aspects is mainly due to the maintenance and visual aspects of the bathrooms, where women consider giving birth in the tubs. The bathtubs do not comply with the current legislation regarding dimensions, the position in relation to the toilet makes it difficult for professionals to work at the time of delivery and the conditions of conservation bring insecurity to women, although many still choose to go through with the delivery in the water. The condition of the coating in these facilities is also very compromised, not contributing to the good perception or safety in the use of the environment.
Illustration 18 - Bathrooms inside the Normal Labor Rooms
 |
 |
Photo credit: Cristiane N. Silva (2018)
- Employee evaluation: Employees recognize that, even though there are various problems to be addressed regarding their own comfort and working conditions, they feel satisfactorily met by the facilities of the Birth Center in the aspects considered. This item is directly related to their conditions of comfort, how they see the space as a facilitator of the work process and the appropriation through the application of knowledge and experience of professionals. It interferes with the related aspects, but with a vision directed exclusively to the conditions found and perceived by the multiple teams of employees. It also interferes with issues related to personal space, control and privacy of employees, observing the conditions of the environments given to these professionals.
The spaces of the Center are primarily intended to provide healthcare service, which is very good, but requires a closer look at comfort, work and equipment intended for professionals who provide services. Issues such as lack of maintenance and the need to expand some sectors at the Birth Center to better serve the public were mentioned by users who took part in the research and those who didn't, but said so in informal conversation during the visits, which was understood as the result of administrative issues and lack of funding to meet the needs of the unit, but that do not prevent the Center from providing care, even if they influence everyone's perception concerning the available working conditions.
Illustration 19 - Patient Medical Record Station
 |
 |
Source: Photographs provided by Adriana Medeiros (2018)
- Accesses: From all the items from the evaluation forms, this was the one that received the lowest grade. The questions refer to the conditions of access, accessibility and safety of users, especially in the case of pregnant women, who may already be in labor, and families with newborn babies. They directly interfere with customers' perception of the possibility of getting to and from the site safely and easily. Besides the distance from the main road, another fundamental issue that affects perception is the immediate surroundings of the Birth Center, with arid and very empty streets, besides the countless reports of public insecurity. The difficult access and insecurity affect not only the clients, but the professionals and service providers working in the Center.
4. Considerations regarding the "model" and the Center
The Birth Center model, represented in this study by David Capistrano Filho Birth Center, shows, through the results of the evaluations performed, that it is a synthesis of the aspects presented in the theories, recommendations and normative for environments intended for humanized birth, This opinion is shared not only by women, but also by guests and staff.
The Center also makes it clear that, despite the formal aspects that make a huge difference, the ambience does not rely only on the physical structure. In this childbirth care unit, which has a deficient physical structure, and needs not only maintenance but also expansion, the working methodology employed, the dimension of empathy assimilated, the knowledge and recognition, all working together, make a huge difference to the final result of the service provided by those who work there welcoming those looking for care.
This model is not limited to the constructive and tangible aspects of built facilities, but to a composition of these with the form of care, with the familiarity generated by the protocols of information and clarification, for allowing privacy, but encouraging coexistence, to provide freedom of flow, for becoming part of the everyday life of families who seek the Center during pregnancy and after birth. The Birth Center becomes everyone's home; the birth returns to its origin and the family. Families go back to follow up on future pregnancies, children who were born there can be seen around the house, accompanying other bellies that bring new children. They join the local community, working together to help through the most difficult phases of lack of funds or marching to maintain the service, which is constantly threatened with termination, they take part in a community organization (ReParto - David Capistrano Birth Center Support Network), which comprises employees, friends and users of the Birth Center. They own and establish the territory.
The work processes and the typology of care provided at the Center result from written protocols and experiences of the healthcare team, to which many professionals belong since before the inauguration. They are the result of knowledge gathered throughout the existence of the house and the deliveries performed there and from all the experience, safety and confidence imparted by the professionals regarding the quality of the work performed. The trust invoked by the healthcare team acts alongside with the empathy and the environment, increasing the feeling of physical and emotional well-being of individuals, positively influencing the perception of the environments as a whole, in order to minimize aspects that could be perceived negatively, which would result from the maintenance difficulties currently faced by the Birth Center.
The Birth Center also meets the prerogatives of the humanization of childbirth on the need to take back the typical labor to recognizable environments resembling a home birth, but with immensely fewer possibilities of complications, due to the care provided for the women and the experience and knowledge of the obstetric nurses, capable and legally qualified for their work. It is up to us to recognize the need for a major process of change for this Birth Center model not only to be accepted, but also multiplied as an important tool for the necessary changes in the model of childbirth in the country. Therefore, it is also as important to recognize it as an important aid in reducing maternal and neonatal mortality, which implies also changing the culture of cesarean section, by expanding information and clarification on the subject, not only to the general population, but even to managers and health professionals, who still question the safety of this type of delivery and birth care unit.
Footnotes
[1] "For sensitive environments in the birthplace. Perception and subjectivity in the normal birth centers".
[2] Normal birth is often used as a synonym for "vaginal birth". When it comes to natural childbirth, in addition to vaginal delivery, it should be emphasized that the baby is born without medical intervention, such as anesthesia, painkillers or inducing drugs.
[3] Fetal dystocia is the occurrence of fetal size or position abnormalities, resulting in difficulties in childbirth. The diagnosis is made by clinical examination, ultrasound or by response to the evolution of labor.
[4] Episiotomy is an incision made in the perineum to enlarge the birth canal. This is one of the main condemned interventions in the good birth practices established by the WHO (WHO, 1985).
[5] David Capistrano da Costa Filho has a PhD in public health and was a leader of the student movement. His constant participation in National Health Talks granted him national recognition for his innovative nature of thinking about health. His importance for the public health area is mainly due to his contribution to the establishment of SUS. He was responsible for the creation of the first Birth Center (AZEVEDO, 2008).
[6] The Birth Plan can be a either a letter or list in which the pregnant woman determines what she would like and would not like to have at birth to ensure the quality of care and experience. Pregnant women are advised about the possible scope and limitations of requests at group meetings during prenatal care.
References:
AZEVEDO, L.G.F. Estratégias de luta das enfermeiras obstétricas para manter o modelo desmedicalizado na Casa de Parto David Capistrano Filho. Dissertação apresentada, como requisito para obtenção do título de Mestre, ao Programa de Pós-Graduação em Enfermagem da Universidade do Estado do Rio de Janeiro. 2008.
BITENCOURT, F. Arquitetura do Ambiente de Nascer: Investigação, reflexões e recomendações projetuais sobre conforto humano em centros obstétricos. Tese de doutoramento em arquitetura apresentada ao Programa de Pós-graduação em Arquitetura da faculdade de Arquitetura e Urbanismo da Universidade Federal do Rio de Janeiro - PROARQ/FAU/UFRJ. 2007.
BITENCOURT, F. e COSTEIRA, F. Entrevista. Entrevistador: Cristiane N. Silva. Rio de Janeiro - RJ, 2010. 1 arquivo .mp3 (110 min.).
BRASIL. Ministério da Saúde. Programa de assistência integral à saúde da mulher. p.7-12 2000.
_______ Regulamento Técnico para Funcionamento dos Serviços de Atenção Obstétrica e Neonatal - Resolução da Diretoria Colegiada - RDC N° 36, de 03 de junho de 2008. Agência Nacional de Vigilância Sanitária. Brasília - DF. 2008.
_______ Oficina de Ambiência para o Parto e Nascimento. Rede Cegonha. HumanizaSUS. Política Nacional de Humanização DAPES /SAS Ministério da Saúde. São Paulo - SP. 2012
COELHO, G. A arquitetura e a assistência ao parto e nascimento: Humanizando o Espaço. Dissertação de Mestrado submetida ao Programa de Pós-graduação em Arquitetura, Faculdade de Arquitetura e Urbanismo, da Universidade Federal do Rio de Janeiro - UFRJ. 2003.
CPDCF - CASA DE PARTO DAVID CAPISTRANO FILHO. Casa de Parto. Disponível em: http://smsdc-casadeparto.blogspot.com/p/quem-somos.html. Acesso em: junho de 2018.
DE VICO. A. F. Avaliação da Implantação dos Centros de Parto Normal no Sistema Único de Saúde. Dissertação apresentada à Pós-graduação em Saúde da Criança e da Mulher, da Fundação Oswaldo Cruz e do Instituto Nacional de Saúde da Mulher, da Criança e do Adolescente Fernandes Figueira. Rio de Janeiro - RJ. 2017
DINIZ, C.S.G. Humanização da assistência ao parto no Brasil: os muitos sentidos de um movimento Ciência e Saúde Coletiva 10(3): 627-637. 2005. Disponível em: http://bhpelopartonormal.pbh.gov.br/estudos_cientificos/arquivos/humanizacao_da_assistencia_ao_parto_no_brasil_os_muitos_sentidos_de_um_movimento.pdf. Acesso em junho de 2017
FERREIRA, K.A; MADEIRA, L.M. O significado do acompanhante na assistência ao parto para a mulher e familiares. Enfermagem Obstétrica, Rio de Janeiro, 2016 jan/abr; 3(1): e29. p.1. Disponível em: http://www.enfo.com.br/ojs/index.php/EnfObst/article/download/29/28. Acesso em dezembro de 2018.
KOMURA. L.A.; DE SOUZA C.M. Assistência ao parto com a presença do acompanhante: Experiências de profissionais. Invest. Educ. Enferm. 2007; (25)1: 74-81. Disponível em: https://www.redalyc.org/pdf/1052/105215404008.pdf. Acesso em dezembro de 2018.
MACHADO, N.X.S; PRAÇA, N.S. Centro de parto normal e assistência obstétrica centrada nas necessidades da parturiente. Ver. Esc. Enferm USP 2006; 40(2):274-9. Disponível em: http://www.scielo.br/pdf/reeusp/v40n2/16.pdf. Acesso em julho de 2018.
PAZ, L.S.; FENSTERSEIFER, L.M. Equipe de enfermagem e o acompanhante no parto em um hospital público de Porto Alegre. Revista Interdisciplinar NOVAFAPI, Teresina. v.4, n.1, p.9-13, Jan-Fev-Mar. 2011. Disponível em: https://revistainterdisciplinar.uninovafapi.edu.br/revistainterdisciplinar/v4n1/pesquisa/p1_v4n1.pdf. Acesso em dezembro de 2018.
PEREIRA, A.L.F.; MOURA, A.V. Hegemonia e contra hegemonia no processo de implantação da casa de parto no Rio de Janeiro. Rev. Esc. Enferm. USP. 2009; 43 (4): 872-9. Disponível em: http://www.scielo.br/pdf/reeusp/v43n4/a19v43n4.pdf. Acesso em março de 2018.
PEREIRA, A.L.F.; AZEVEDO, L.G.F.; MEDINA, E.T.; LIMA, T.R.L.; SCHROETER, M.S. Maternal and neonatal care in David Capistrano Filho Birth Center, Rio de Janeiro, Brazil. Revista online de pesquisa Cuidado é fundamental. Capa > v. 4, n. 2 2012. DOI: http://dx.doi.org/10.9789/2175-5361.2012.v4i2.2905-2913. Acesso em fevereiro de 2018.
RODRIGUES, D.P.; ALVES, V.H.; PENNA, L.H.G.; PEREIRA, A.V.; BRANCO, M.B.R.L; SOUZA, R.M.P. O descumprimento da lei do acompanhante como agravo à saúde obstétrica. Texto Contexto Enferm, 2017; 26(3):e5570015. Disponível em: http://www.scielo.br/pdf/tce/v26n3/0104-0707-tce-26-03-e5570015.pdf. Acesso em dezembro de 2018.
SILVA, A.L.C. (2015). Centro de parto normal: Humanizando o Espaço. Revista Especialize On-line IPOG - Goiânia - 9ª Edição nº 010 Vol.01/2015 julho/2015. Disponível em: https://www.ipog.edu.br/revista-especialize-online/edicao-n9-2015/centro-de-parto-normal-humanizando-o-espaco/. Acesso em agosto de 2018.
SILVA, C. N. Aspectos subjetivos dos ambientes de atenção à saúde e sua relação com o ambiente construído. Arquitextos, São Paulo, ano 18, n. 212.05, Vitruvius, jan. 2018 <http://www.vitruvius.com.br/revistas/read/arquitextos/18.212/6867>.
SILVA, C. N. Considerations in the care of pregnant women. IFHE Digest. Revista eletrônica. Edição de 2018. Step House, North farm Road Tunbridge Wells, Kent TN2 TD R. 2018a. Disponível em: https://www.ifhe.info/ifhe-digest
SILVA, C.N. (2018b). Ergonomia aplicada na qualificação da ambiência do espaço de nascer. Revista Sustinere, Rio de Janeiro, v.6, n.1. P 150-174, jan.-jun. 2018. Disponível em: HTTP://dx.doi.org/10.12957/sustinere.2018.33609
WALSH, D., Evidence-based care for normal labour and birth: a guide for midwives. 2007, London: Routledge.
About the author:
Cristiane N. Silva
Architect, PhD in Architecture from UFRJ, expert in Management of Healthcare Networks from Escola Nacional de Saúde Pública Sergio Arouca - ENSP / FIOCRUZ. She is an advocate for Hospital Ambience at the Ministry of Health and helps with hospital infrastructure management services at the Ministry of Health State Superintendence of Rio de Janeiro, besides teaching maintenance management and conservation of healthcare buildings.
Share




Send by e-mail: