Publications IPH Magazine IPH Magazine #16 Risk of infections caused by the presence of the fungus Aspergillus.sp: remodeling hospitals and climatization systems

- An analysis of the sectorization and comfort in contemporary children's hospitals
- "Casinha": The story of the Birth Center in Rio de Janeiro that became a model for humanized labor and resistance to the hardships of public management
- Risk of infections caused by the presence of the fungus Aspergillus.sp: remodeling hospitals and climatization systems
- Health financing systems worldwide
- A pathway for death: the flow and connections between environments and its occupants
Risk of infections caused by the presence of the fungus Aspergillus.sp: remodeling hospitals and climatization systems
Watson Freire Dias
1. Introduction
The fundamental principles that guided us to conceive this article were the risks that environments being remodeled and air-conditioning equipment may pose to inpatients, especially those in intensive care units (ICU). Based on the literature and publications, our focus was to determine the risks posed by microorganisms present in areas where civil works are carried out and if when associated with a precarious climatization system it could lead to a potential harmful effect to health promotion. Moreover, we present and analyze the reports of microbiological assessments carried out in the ICU of a high-complexity hospital in São Paulo.
2. Treatment and indoor air quality at healthcare facilities as an element of healing
In healthcare facilities, especially hospitals, air-conditioning projects must consider every circumstance of the environment and investigate all the demands for each location, and not just the thermal comfort. Air conditioning systems can be an important source of microorganisms. Substantial volumes of physical, chemical and biological pollutants affect workers and inpatients, especially those with depressed immune systems (COSTA, 2007, p. 4).
Environments with low air exchange rates cause a quantitative increase in clusters of airborne chemical and biological pollutants, which therefore harms the health of the population. For that reason, indoor air quality (IAQ) has become a paramount object of research in the area of public health (TURIEL et al., 1983 apud BRICKUS; AQUINO NETO, 1999). We should extra careful with air conditioning systems, seeing that the chances of having undesirable contaminant microorganisms carried in suspension decreases if the air is cleaner. Such risk increases proportionally regarding the rates of airborne particulates (BICALHO, 2010).
The concern regarding air quality, as well as its concept, is applied to every area under climatization, without exception. However, Quadros (2008) highlights the quality of the air in healthcare facilities represents a more critical issue, since it can have a direct impact over the speed of patient recovery, as well as over the prevention of nosocomial infections. Related studies are even more important when considering the treatment units for cancer and immunosuppressive diseases, which affect patients' immune systems (QUADROS, 2008).
Nowadays, most patients with access to medical care gets better. Nonetheless, there is a part of the population that suffers the unintentional consequences of healthcare, such as the infections related to health assistance (SINGH; BRENNAN; BELL, 2008).
If we consider all hospital environments, the ICU is one of the most conducive to give rise to infections and bacterial resistance, since patients are more exposed to hazardous procedures and the peculiar conditions of these units. The contamination caused by microorganisms present in the hospital environment benefits from the susceptible condition of the patient, considering the therapeutic and diagnostic approaches that can impair the mechanical barriers of the skin and mucosae (BARBOSA, 2010 apud MORAES; RAU, 2011).
The airborne spread of fungal spores through hospital ventilation systems and clothes contaminated by air disruption are among the most frequent fungal infections. They are highly accountable for morbidity and mortality among immunocompromised patients (FRARE, 2009).
When discussing the reasons for nosocomial through the air, Dias, Costa and Pataro (2014, p. 31) show that:
The importance of conducting a microbiological assessment of the ambient air is justified due to the outbreaks of fungal and bacterial infections often associated with construction sites and remodeling in hospitals. A study carried out by VONBERG & GASTMEIER (2006) investigated 53 outbreaks caused by invasive Aspergillosis infection and found that 49.1% of probable or possible cases of Aspergillus spp. were related to construction and remodeling in hospitals, and 17% were related to refrigeration problems. The most common source of transmission was the air, and the lower respiratory tract was the main site of infection, followed by surgical and skin wound infections.
Frare (2009) adds to the aforementioned statement when it makes a reference to Frech (2005), describing an increase in cases of Aspergilose among immunosuppressed patients during remodeling processes within the hospital areas besides the non-reliable maintenance of air filter. He emphasizes then the importance of having total integration in the work and communication processes between the commissions that control nosocomial infections and the engineer areas, aiming at the prevention against such infections and avoiding outbreaks in hospitals.
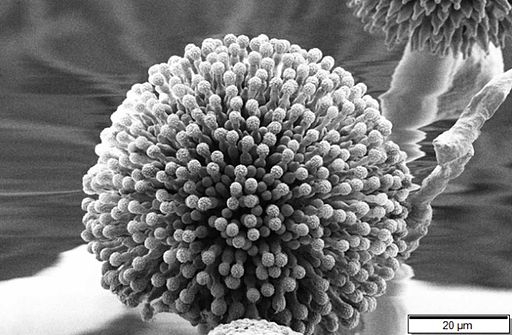
Karman (2011) points out that Aspergillus fungus, with an average diameter of 2 to 3.5 µm, including its spore, is resistant to dehydration and may remain suspended in the air indefinitely if associated with dust and moisture.
Picture 1 - Aspergillus
Credit: Mogana Das Murtey and Patchamuthu Ramasamy [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)
The modern technologies for climatization systems can improve indoor air quality, since it is possible to design suitable filtration and temperature control systems, which you can regulate to meet various specific conditions. However, they should be employed with full awareness of the adverse impacts on human health. Although filters remove unwanted particles and breathable particles from outdoor air, they enable an environment that helps develop a multitude of bacteria and other infectious agents. As a result, it is necessary to estimate the costs for the maintenance of the building to monitor and replace filters regularly (STERLING; COLLET; RUMEL, 1991).
Among the various diseases caused by fungi and bacteria that spread through air conditioning systems in hospitals and health facilities, the Aspergillus is one of the main agents responsible for fungal infections, presenting high mortality rates, between 68% and 95% (FRARE, 2009). As Bernal (2015) said:
Aspergillus spp. is an opportunistic saprophyte widely spread across nature. It can cause a wide range of diseases, from allergies to invasive infections in humans. Invasive Aspergillosis (AI) is the most serious infection caused by Aspergillus spp. It affects mainly the lungs of immunosuppressed patients and may spread to deep organs. (BERNAL, 2015, p. 315).
Aspergillosis is one of the most recurrent fungal infections in immunosuppressed patients, besides being the main cause of death among such patients. They get the disease after inhaling: fungal spores found in hospital ventilation systems; air contaminated by construction sites and remodeling; dust and contaminated materials. Units treating cancer and transplants, especially those without air filtration and air renewal systems, are considered high-risk environments for Aspergillosis outbreaks (FRARE, 2009).
3. Testing the quality of the air inside the ICU of a specialized high-complexity hospital
To test the presence of Aspergillus fungus in the sector, we will present the results from microbiological tests of air harvested in the ICU common treatment area at a public, state-managed, medium-sized specialized high-complexity hospital, located in the city of São Paulo.
The ICU of this hospital was remodeled in the first half of 2017, the process was completed in July of the same year. For the research, we have strategically chosen three samples of air: the first one from December 2016, under normal conditions, before remodeling had begun; the second, shortly after the work had finished, in August 2017; and the last one in November. In August, the thin and absolute filters were replaced in the air conditioning system that supplies to the building. The entire system receives preventive and corrective maintenance regularly, when required, which is overseen by a professional mechanical engineer. Prior to remodeling, an essential and contingent plan was prepared with the Institution, aiming at impacting as little as possible patients and other departments in the hospital.
Pictures 2 and 3 - Replacing F7 saturated bag filters, August 2017
 |
 |
Credit: Personal collection.
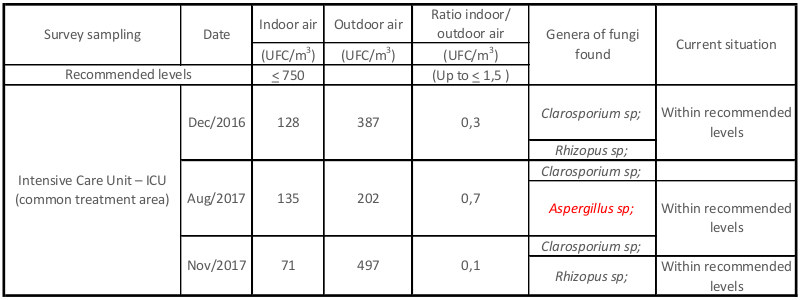
The analysis concerning the quality of indoor air were carried out following the recommendations put forward by the Brazilian Association of Technical Standards (ABNT) ISO/IEC 17025, NBR 10719 and by Ruling - RE n. 09, from MS/ANVISA, on 16 January 2003. Based on the regulatory standards, here there are the results obtained from our three tests:
Table 1 - Technical Standard #1
Source: Indoor air quality report after testing. Personal collection.
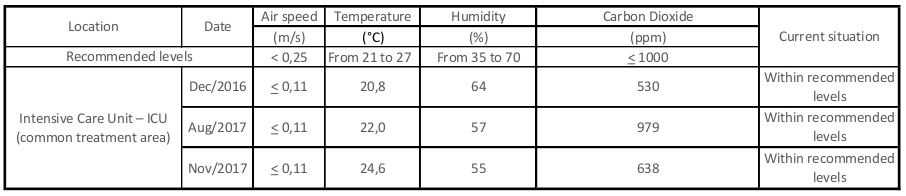
Table 2 - Technical Standard #2 and #3
Source: Indoor air quality report after testing. Personal collection.
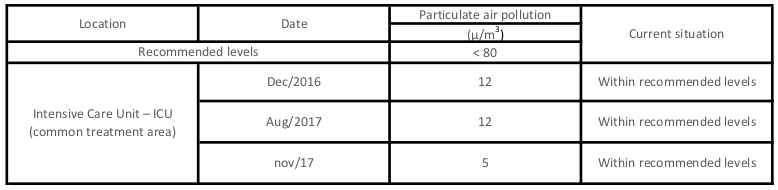
Table 3 - Technical Standard #4
Source: Indoor air quality report after testing. Personal collection.
Regarding the aforementioned Technical Standards, all results are within acceptable levels from a quantitative standpoint. On the other hand, from a qualitative viewpoint, Table 1 indicates the presence of fungus Aspergillus in the environment almost at the same time the works were being carried out.
As a consequence, and based on theory, it is possible to verify the presence of this microorganism is directly related to the intervention period, corroborating what Karman states (2011, p. 151):
The rowdiness caused by construction and remodeling works, especially in healthcare facilities, can release dust with airborne spores of Aspergillus fungi, which are potentially lethal for immunosuppressed patients. The Aspergillus fungus, which is 2 to 3.5 µm (diameter), is found on the soil, at moist environments and in rotting vegetables. It can also be found in ventilation systems that are not operating properly: air filters, window air conditioners, suction fans, false ceilings, acoustic ceilings, construction sites, exposed doors or windows, hospital vacuum cleaners, ornamental plants, pigeons etc. The dust from neighboring work sites can also affect healthcare facilities since the Aspergillus is sporulated and airborne (airborne bacterium). The humidity of an environment also contributes to its proliferation. Thus, equipment and instruments colonized with the fungus, when stored in humid environments, might become a source of infection.
Even though the amount of fungus we found respects the standards, we emphasize that taking precautions in the areas under work is essential to keep the maintenance of climatization systems updated and, thus, avoiding that such systems ever become potentially harmful agents. For this intervention, specifically, the hospital technical team did not find infections whose main cause was the Aspergillus. Nevertheless, the fungus remains, indeed, a threat, especially to patients and others, who visit or work at the hospital.
4. Conclusion
In this paper, we concluded that remodeling hospital environments increase the circulation of Aspergillus.sp, with greater risk to the ICU sector. Therefore, the judicious assembly of physical barriers and, above all, the proper maintenance of climatization systems can prevent this fungus from accommodating and spreading itself through the ducts, which would represent potential risks to patients. In the case we have presented, it is not possible to assert the source of the microorganism was directly associated with the climatization system, however, the maintenance carried out in the air conditioning equipment certainly helped isolate and stop the growth of Aspergillus.sp fungus in the environment.
Indeed, it becomes clear that the topic discussed here is very relevant and deserves our special attention. Above all, it is a warning against all threats that come with having around a fungus with higher pathogenic risk. Moreover, it justifies a more thoroughly examination focusing on hospital application by professionals who share a sensitive look towards these issues and envision the future of healthcare buildings to effectively provide healthcare assistance.
References
BERNAL, M. L.; ALASTRUEY, I.; CIENCA, E. M. Diagnostics and susceptibility testing in Aspergillus. 2015. Disponível em: <https://www.id-hub.com/2017/02/24/diagnostics-susceptibility-testing-aspergillus/>. Acesso em: 12 dez. 2017.
BICALHO, F. de C. A Arquitetura e a Engenharia no controle de infecções. Rio de Janeiro: Rio Books, 2010. 135 p.
BRICKUS, L. S. R.; AQUINO NETO, F. R. de. A qualidade do ar de interiores e a química. Química nova, v. 22, n. 1, p. 65-74, 1999.
COSTA, M. R. Recomendações para o controle de qualidade do ar climatizado. 2007. 12 f. Tese (Doutorado) - Curso de Comissão de Controle de Infecção Hospitalar, Universidade Católica de Goiás, Goiânia, 2007.
DIAS, R. S.; COSTA, P. D.; PATARO, C. S. Ambiente hospitalar como fator de risco para a ocorrência de infecções oportunistas por Staphylococcus Aureus Multirresistentes. Periódico Científico do Núcleo de Biociências: Centro Universitário Metodista Izabela Hendrix, Belo Horizonte, v. 4, n. 7, p. 27-35, ago. 2014.
FRARE, F. Infecção hospitalar por aspergillus: análise da implantação de uma unidade de ambiente protegido. 2009. 28 f. Trabalho de Conclusão de Curso (Graduação) - Curso de Enfermagem, Universidade Federal do Rio Grande do Sul, Porto Alegre, 2009.
KARMAN, J. B. Manutenção e segurança hospitalar preditivas. São Paulo: Estação Liberdade, 2011. 437 p.
MORAES, F. M.; RAU, C. Infecções relacionadas à assistência à saúde (IRAS): impacto na saúde e desafios para seu controle e prevenção. 2011. 17 f. Monografia (Especialização) - Curso de Pós-graduação em Vigilância Sanitária, Pontifícia Universidade Católica de Goiás, 2011.
QUADROS, M. E. Qualidade do ar em ambientes internos hospitalares: parâmetros físico-químicos e microbiológicos. 2008. 135 f. Dissertação (Mestrado) - Curso de Engenharia Ambiental, Universidade Federal de Santa Catarina, Florianópolis, 2008.
SILVA, E. B.; GOMES, S. R. Ar-condicionado: herói ou vilão em unidades de terapia intensiva? REINPEC: Revista Interdisciplinar do Pensamento Científico, Itaperuna, v. 1, n. 1, p. 222-232, jan. 2015.
SINGH, N.; BRENNAN, P. J.; BELL, M. A compedium of strategies to prevent healthcare-associated infections in acute care hospitals: um compêndio de estratégias para a prevenção de infecções relacionadas à assistência à saúde em Hosp. Infection Control And Hospital Epidemiology, Cambridge, v. 29, n. 10, p. 901-994, out. 2008.
STERLING, T. D.; COLLET, C.; RUMEL, D. A epidemiologia dos "edifícios doentes". Revista Saúde Pública, São Paulo, v. 25, n. 1, p. 56-63, jan. 1991.
References Concerning the Technical Standards
ANVISA - Agência Nacional de Vigilância Sanitária. Importância dos projetos de sistemas de climatização em estabelecimentos assistenciais de saúde (EAS). Brasília: Anvisa, 2009. 4 p.
______. RDC nº 50 Normas para projetos físicos de estabelecimentos assistenciais de saúde. 2. ed. Brasília: Anvisa, 2004. 160 p.
______. Resolução RE nº 09, de 16 de janeiro de 2003. Diário Oficial da União, Orientação técnica elaborada por Grupo Técnico Assessor sobre padrões referenciais de qualidade do ar interior em ambientes climatizados artificialmente de uso público e coletivo. Brasília, DF: Imprensa Oficial, 20 jan. 2003. n. 14, Seção 1, p. 35-37.
BRASIL. Constituição (1992). Portaria nº 930, de 27 de agosto de 1992. Infecção Hospitalar: Ministério da Saúde. Disponível em <http://www.ebah.com.br/content/ABAAAAr90AL/portaria-n-930-27-agosto-1992>. Acesso em: 21 jun. 2017.
BRASIL. Constituição (1998). Portaria nº 3.523, de 28 de agosto de 1998. Regulamento Técnico. Procedimentos de verificação de limpeza, remoção de sujidades por métodos físicos e manutenção do estado de integridade e eficiência de todos os componentes dos sistemas de climatização.
Share




Send by e-mail: