Publications IPH Magazine Magazine IPH Nº19 Design for health environments: how neuroscience applied to architecture can contribute to the health and well-being of its users
- Editorial Magazine IPH Nº19
- From Hospital Architecture to Architecture for Health
- Design for health environments: how neuroscience applied to architecture can contribute to the health and well-being of its users
- Jarbas Karmans experience during his SESP Years
- Evolution of hospital building, its alignment with medical sciences and patient care in the city of São Paulo
We spend most of our time in the built environment and are often unaware of how it can positively or negatively impact our quality of life, physical and mental health. There are many studies in the field of neuroscience that provide evidence of the impact of architecture on our brain through our senses. The stimuli caused by the environment are captured by our receptor cells that lead to our nervous system causing the sensations, emotions, feelings that shape our behavior. This work aims to describe aspects of neuroscience with a focus on health environments through bibliographic research and application in architectural projects. These aspects are applied environmental strategies such as biophilia, lighting and acoustic comfort considering the five senses as the main access route to our brain. Through the studies of neuroarchitecture it is possible to design environments that can improve the performance, wellness, social relationships, and recovery of its users.
Keywords
neuroscience, neuro architecture, brain, biophilia, senses, behavior
2. Introduction
Villarouco (2021:9) brings reflections on the spaces we inhabit and the number of environmental stimuli we receive and guide our emotions, thoughts, and behaviors. Elements such as light, color, sound, nature, texture, and smell can affect our well-being, often unconsciously.
According to neuroscientist Tieppo, (2019, p.1), the brain controls every aspect of human life, and it becomes increasingly clearer that everything we see, hear, smell, digest, talk, feel and think depends on how the brain reacts. Including how we act and behave, our beliefs, memories and desires, our motivation and even our own identity
By this logic, architecture can influence how the brain reacts to stimuli provoked in the built environment. According to Eberhard (2009, p.753), most neuroscientists believe architecture is a profession concerned with beauty and aesthetics, which we perceive by the visual system of harmony, symmetry, and proportions. However, architecture is more than aesthetic, it needs to meet the functional needs of users, have elements such as lighting and natural ventilation. He suggests that classrooms should provide cognitive activities, inpatient rooms should assist in patient recovery, and that work environments should be more productive.
Nanda (2005, p.164) descreve que um bom ambiente sensorial não é aquele que desperta todos os sentidos intensamente, mas que proporciona uma sintonia entre eles, ou seja, não se trata de estética e aparência, mas, sim, de estética da experiência. O nosso sistema nervoso é quem processa os estímulos recebidos a todo instante, tais como: o som do vento, a rua movimentada, os pássaros, a conversa dos colegas de trabalho, os carros que passam na rua, o cheiro de café ou de alguém fumando, o gosto doce de um brigadeiro, as cores, o frio ou o calor.
Nanda (2005, p.164) describes that a good sensory environment is not one that awakens all the senses intensely, but that provides harmony among them, that is, it is not about aesthetics and appearance, but rather the aesthetics of the experience.
Our nervous system is responsible for processing the stimuli received at all times, such as: the sound of the wind, the busy street, birds, conversations of co-workers, cars passing along the street, the smell of coffee or someone smoking, the sweet taste of recently baked apple pie cake, colors, the cold or the heat.
Often, we cannot perceive these stimuli consciously. Levitin (2015, p.37) describes how the human brain has evolved to hide from us certain things we don?t pay attention to. We have a cognitive blind spot, where the brain completely ignores what is not a priority at that moment, even if it is in front of our eyes. According to him, cognitive psychologists call this blind spot blinding by negligence. In this sense, knowing and applying neuroscience to architecture, commonly called neuroarchitecture, helps us build more efficient and purposeful environments, promoting well-being to its users.
2. Methodology
Therefore, the goal was to understand how our nervous system works and how we can, through neuroscience studies, design spaces intend to contribute to the well-being and quality of life of people in health environments, such as hospitals. The result of the research aims to awaken new perspectives towards design, focusing on user?s experience, whether it is a patient, companion, or employee. The research focused on knowing our nervous system and applying environmental strategies, such as: biophilia, lighting and acoustic comfort, considering the five senses. Ultimately this work wishes to establish a multidisciplinary approach to the fields of medicine, biology, architecture, among others.
3. Understanding the nervous system
According to Preuss (2014, p.1), humans have very different cognitive abilities in comparison to other creatures, thanks to a few unusual characteristics of our brain, such as the fact that it weighs, on average, 1.3 kg, which is very large for our body. Most of this difference in brain size is due to the evolutionary expansion of the cortex, a region that performs sophisticated cognitive functions, such as language, consciousness, and problem solving. The size of the cortex is part of what makes man different from other animals.
According to BrainFacts.org (2012, p.1), the nervous system is divided into two parts: central nervous system and peripheral nervous system. Both works together so the body can properly share the sensations and their needs. The central nervous system is formed by the brain and spinal cord. The brain is inside the skull, and the spinal cord is protected by the spine. The peripheral nervous system consists of nerves that run through the entire body. The brain sends its messages through the spinal cord to the peripheral nerves of the whole body, in addition to control the muscles and internal organs. The peripheral nervous system is subdivided into somatic and visceral. The somatic is composed of neurons that connect the central nervous system to parts of the body that interact with the outside environment. The visceral is composed of neurons that connect the central nervous system to the internal organs.
The peripheral nervous system is also subdivided into two parts: sympathetic and parasympathetic. The sympathetic system applies energy and resources for moments of stress and excitement; while the parasympathetic saves energy and resources during the state of relaxation, such as sleep
The nervous system is an information processing system. There is information continuously coming and going, like cars running at great speed on highways. Through the nervous system, we receive information about the external environment ? through vision, hearing, touch, smell, taste ? and the internal environment, our interior ? such as pain, body position, thoughts, emotions, memories, information of the viscera. Thus, we select, process, and combine the information, producing answers from it. That is, the nervous system receives signals from the environment, from all parts of our body and responds to the stimuli received, producing an action, a movement, a behavior (TIEPPO, 2019, p. 111).
Regarding the conscious perception of the built environment undergone by our brain through sensory stimuli, Paiva (2019, p. 565) points out that to process information consciously, we use less than 1% of our unconscious processing capacity, according to Eagleman. Therefore, most stimuli will affect individuals on a subconscious level. Although people may be affected by stimuli, they are not necessarily aware of the effect.
Individuals are in constant active interaction with many environments around them. A warm room can cause people to sweat, feel uncomfortable and unable to concentrate. A dark room can make people feel scared, alert, and unable to relax. A bright classroom with natural light can help students be attentive to the class. The environment always affects its occupants on some level. This interaction can be called architecture and individual relationship. Spaces can change people (architecture and individual),
Individuals are in constant active interaction with many environments around them. A warm room can cause people to sweat, feel uncomfortable and unable to concentrate. A dark room can make people feel scared, alert, and unable to relax. A bright classroom with natural light can help students be attentive to the class. The environment always affects its occupants on some level. This interaction can be called architecture and individual relationship. Spaces can change people (architecture and individual), and people can change spaces (individual architecture). Therefore, this relationship is a two-way street (PAIVA et al, 2019, p. 565).
Based on the knowledge of neuroscience and application to architecture, the term neuroarchitecture has been studied in more depth. It is believed that the beginning of neuroscience applied to architecture, according to Carbone (2021, p.13), occurred with the studies of Fred Gage, a neuroscientist who, in 1998, discovered that the brain continued to produce hormones in adulthood, which led him to be interested in how the environment influences the structure and functioning of our brain. Alongside John Eberhard and other professionals, Gage founded ANFA (Academy of Neuroscience for Architecture). For him, the design of spaces in the 21st century needs to improve our well-being, improve our performance, and reduce stress and fatigue in cities.
Subsequently, it will be presented environmental strategies based on the study of neuroscience, which architects and designers can use as a design tool to enrich environments, minimize short- and long-term negative effects and enhance positive effects. Strategies to stimulate the senses (vision, smell, taste, touch, hearing) will be presented in correlation to topics such as biophilia, lighting, acoustic comfort and how they can be applied to health environments in a practical way. In addition, the strategies will be depicted through some illustrations of projects under study and of environments already built.
4. Stimulating the senses
The information received from the environments varies, but the perception is the same. Natural light, for example, throughout the day, suffers variations in temperature and color. But what we perceive around us does not change. One of the functions of built environments is to promote emotion. ?We are, above all, beings moved by emotion [...] The emotion is like a roller coaster, it leaves us ungoverned at certain times, but it also boosts us. We are emotional beings.? (TIEPPO, 2019, p.167).
Neuroarchitecture, as a study that also seeks to understand the spatial understanding of its users, so that they can get a better experience in relation to the projected environments, nourishes the awakening of mental triggers linked to sensations, emotions, and behaviors in their search for results. Knowing how to naturally access this challenging and rich system of human integrations, aiming to give users positive experiences in the face of living with environments, makes design practices efficient in their most symbolic purpose: to promote an empathic experience to those who are inserted in these specialties (CRIZEL, 2020, p.42).
The part of the brain that produces emotion is the limbic system ? Tieppo (2019, p.167) defines it as the emotional system ?, which is present in various parts of the brain, processes stimuli and responds automatically to them. It provides quick responses to environmental demands. The limbic system was developed throughout the evolutionary process to be able to anticipate situations that require rapid responses, such as escape, attack, and survival. The situations of greatest emotion are strongly recorded in the memory, so our nervous system recognizes them and anticipates the reactions.
Tieppo (2019, p.116) explains that to feel some information, consciously or unconsciously, sensory receptors must be activated. This set of receptors is called somesthetic or somatosensory system. Somesthesis includes the five senses of our body, such as temperature when touching a surface, pain, pressure, and proprioception.
Such quotes show that the nervous system is influenced by the environment, causing emotions, and shaping human behavior. These emotions are produced by the limbic system, which receives and processes information by the senses: vision, hearing, smell, taste, and touch. Next, we will contextualize how senses are impacted by the built environment.
4.1. Vision
According to Tieppo (2019, p.132), vision relies on receptors that respond to light, energy, and electromagnetic energy. Such receptors are called photoreceptors and are in the retina, divided into cones and rods. Cones are sensitive to three light spectra (green, red, and blue). Rods are sensitive to black and white tones and help you see when there is less light.
The electrical stimulus is taken to some places of the brain, according to Villarouco (2021, p.106), having as first destination the hypothalamus, responsible for regulating the body metabolism and the synchronization of the biological clock, that is, day and night cycle. It is at this point that cones and rods, as mentioned above, begin to act. In the dark, rods are triggered, and in low light the body tends to feel drowsiness and lack of concentration, guided by the biological clock.
Natural and artificial light are great examples of the direct impact of the physical environment on metabolic regulation [...] without the conscious perception of the individual. Through light, the brain synchronizes much of its operation with the external world (circadian rhythm) to cover the 24-hour period in which biological cycle activities take place. Light also regulates physiological and psychological rhythms, directly affecting wakefulness and sleep, hormonal secretion, cellular function, and genetic expression (CRIZEL, 2020, p.274).
Sunlight is the example of lighting that respects the biological rhythm of the human body: by day it emits a more bluish light and, as nightfall, a more yellowish light.
However, modern society lives excessively within built environments, under the influence of artificial lighting, computer, and cellular screens, causing important behavioral changes. In environments where individuals cannot have a sense of day or night, their biological clock loses control of the system for which it is responsible, according to Filho (2018, p. 30).
Red light helps maintain or increase the level of mental activity without suppressing the production of melatonin, a hormone that regulates sleep, unlike blue light. Other studies had shown that bluish lights can reduce the production of melatonin, released by the pineal gland, located at the base of the brain. Melatonin helps regulate circadian rhythm, varying phenomena such as heart rate and sleep that fluctuates in periods of approximately 24 hours. More blue light and less melatonin could leave the body more vulnerable to developing tumors, in addition to deregulating sleep. Those who must stay awake to work at night may feel a little more sleep under red light, but the body is likely to suffer less damage (FIORAVANTI, 2009, p.1).
In a study carried out at Brigham and Women?s Hospital, in Boston, USA, by Rahman et al (2014, p.1), volunteers were tested with exposure to two types of light: bluish and greenish. They all had normal physical and psychological examinations, besides having tested negative for color blindness testing. They were monitored for seven days before the test, with a sleep period of eight hours a day, and could not consume any type of medication, supplement, caffeine, alcohol, or nicotine. During the test, they performed their daily work activities for six and a half hours with a blue light on. It was observed that, during this time, they had higher level of concentration, more keen attention and brain waves that suggested they were in a state of alertness. On the other, the greenish light did not result in any significant difference. The research also concluded that the exposure to blue light at night increases alertness, but suppresses the production of melatonin, a hormone produced by our body and whose main function is to regulate the circadian cycle.
Applying this result to health environments, such as hospitals, which operate 24 hours a day, blue light during the day helps the clinical staff to perform their activities in a state of alertness, focus and concentration. At night, this light can be used to keep professionals focused, however, carefully, so as not to interfere in the circadian cycle. For the patient, reducing the amount of light in the hallway minimizes light interference within inpatient rooms or ICU bed, avoiding interruption of patient?s melatonin production during sleep.
In places destined for hospitalization, where user can stay for many hours or days, good conditions of artificial lighting and a view of the external environment can bring comfort, in addition to the important perception or orientation of time in the face of the circadian cycle. For emergency environments, operating rooms, intensive care units and other critical areas, excessive lighting over the visual impact can result in relevant emotional discomfort, producing irritation and stress, emotions that reduce the quality of care (ANVISA, 2014).
Therefore, it is very important to have natural lighting, both for the patient and for health professionals. Artificial lighting must follow parameters according to standards and be sized for the type of environment and activity to be developed. Also, when possible, it should have dimerization to control light intensity.
According to the ANVISA standard (2002), for environments such as inpatient rooms and ICU beds, in addition to direct artificial lighting and natural lighting, it is mandatory to have emergency lights on the wall, for patient?s spatial orientation at night on the way to the bathroom. Such light can neither influence sleep, nor melatonin production. Therefore, it cannot present blue light spectrum, according to the abovementioned study. In illustration 1, you can see a lighting installed on a footer, which is lit at night and allows spatial identification of the room, providing safety for the patient when getting up. In the ceiling, the lighting is dimerizable, being lit at the highest intensity only during the medical or nursing procedure. The patient and his/her companion are free to regulate the intensity of light according to their needs.


The relations established between human beings and nature have fostered significant changes in the perception and representation of natural elements along their evolutionary path. Relationships, initially instigated by survival instincts, were transposed into domination and control with the advent of agriculture. However, the technological innovations resulting from this did not extinguish the need for the connection between biotic and abiotic elements conditioning the homeostasis of ecosystems, thus demanding, after a short period of withdrawal ? corresponding to less than 5% of human existence ? the gradual resumption of positive attitudes linked to nature (ZANATTA, 2019, p. 950).
Man?s relationship with nature is called biophilia. This concept, coined and popularized by biologist Edward O. Wilson, in his book Biophilia, means humans? innate tendency (of any age, location and culture) to develop an emotional connection with life and living processes (FONSECA, 2009, p. 602).
The results suggest that stressed individuals feel significantly better after exposure to nature scenes, rather than urban scenes without elements of nature. Compared to the influences of urban scenes, the salient effect of nature?s exhibits was to increase Positive Affection - including feelings of affectionate friendship, playful and exaltation. The increase in positive affection produced by nature scenes is consistent with the discovery that nature?s exposures have also significantly reduced the Awakening of Fear (ULRICH, 2007, p. 17).
According to Gressler (2013, p. 489), Roger Ulrich conducted a study at the Pennsylvania Hospital between 1972 and 1981, in which patients with the same clinical condition underwent the same surgery and were placed in hospital beds for recovery: half in rooms overlooking nature and half overlooking a brick wall of the neighboring building. Patients overlooking nature had shorter post-surgical hospitalization and used fewer analgesics. The results of this research suggest that only a glimpse of nature can enable the recovery of stress.
In illustration 3, the inpatient room has a large window and views of a green area. Therefore, it is very important to choose the faces of buildings that will allow inpatient rooms overlooking nature and, when not possible, mimic it with images such as paintings or wallpaper.

Illustration 4 shows the floor plan of the pilotis of a hospital, with commercial galleries, shops, restaurants and living areas, as well as a therapeutic garden. They are paths for mobility where the physical abilities of the patient are tested and improved, with points of contemplation, islands of vegetation to create a differentiated microclimate and shading points.
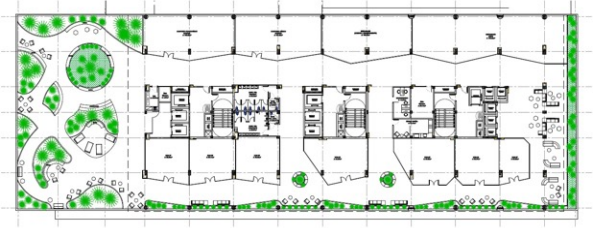
Illustration 4. Gallery and therapeutic garden of a hospital. Source: Illustration produced by the author (2021).

4.2. Hearing
For Tuan (1980, p.10), hearing is not very developed in humans and primates. The eyes get more detailed and accurate information about the environment than the ears, but generally we are more touched by what we hear than by what we see. For many, music is an emotional experience much stronger than the fine arts or sceneries. We are more vulnerable to sounds because we cannot close our ears as we can do with our eyes.
The brain can work on many things at the same time, with overlap and parallelism. This is how our hearing system processes sound: it does not have to wait until it finds out the height of a sound to know where it comes from [...]. Our brain is constantly updating its opinions, especially when it comes to perceiving visual and auditory stimuli, hundreds of times per second, and we don?t even know this (LEVITIN, 2021, p. 90).
NERBASS (2015, p. 108) presents a research on environmental factors that impair the sleep of ICU patients. Among such factors there is the noise caused by the devices connected to the patient, parallel conversations from staff or visitors and companions. Excessive noise has been considered the most sleep disturbing factor in the ICU, with harmful effects not only on the recovery of patients, but also on the health of professionals.
The predominant concept of ICU, for example, are beds arranged in a hall, separated by a curtain, for a better visualization of the patient. However, this model has been proved very inefficient in relation to acoustic comfort. A new concept that has been adopted are closed rooms with glass, allowing visualization of the patient and ensuring a more adequate noise level, as can be seen from illustration 6.

Illustration 6. ICU rooms. Source: Illustration produced by the author (2021).
On the other hand, the presence of music in these environments has been shown, through scientific studies, to be beneficial for ICU patients, for example.
According to Junior research (2018, p.6), there is evidence of reduced symptoms of discomfort, increased positive sensations, facilitation of personal and interpersonal communication, greater sociability, reduction of physical and mental pain, beneficial changes in physiological patterns and body stimulation with the use of music therapy. Among the 35 studies analyzed by him, 14.5% indicate that music helps in the decrease of anxiety; 31,7% recommend the use of music as nursing intervention; 18.4% conclude that music acts in physiological responses; 12.4% refer to music as a viable alternative for sedative and anxiolytic use; and 17.9% conclude that music helps reduce pain. However, 3.2% report that there were no significant results for patients regarding the use of music
From the end of the 20th century, the Ministry of Health established important comfort strategies in the National Policy for the Humanization of Care and Management in the Unified Health System ? Humaniza SUS. Among the recommendations for humanized ambiences, the existence of noise was highlighted, hence the proposal for ?the use of background music in some spaces, such as wards and waiting rooms. In another context, it is also important to consider acoustic protection that guarantees privacy and control of some noises? (BRASIL, 2010, p. 122).
A measure of humanization for hospitalized patients refers to the use of music individually, using disposable headphones. Solution for patient comfort recommended by scientific studies and professionals dealing with the acoustic comfort component. This measure has presented results ?that can regulate mood, reduce aggressiveness and depression? justified because the ?musical hearing process positively affects the release of brain chemicals? (ARAÚJO, 2013:1319APUD BITTENCOURT, 2021, p. 13).
Finishing materials should also be considered as a strategy to reduce noise. There are guidelines regulating the level of noise within built environments. One of them is NBR 10.152, which regulates noise levels for acoustic comfort, whose limits depend on the type of environment and the activity performed.
Bittencourt (2021, p.20) mentions some design aspects for health buildings, in order to enhance noise reduction, such as: choosing the land properly; considering environmental aspects that may impact acoustic comfort; evaluating the impact of natural conditions, landform, topography and geological conditions in the implementation of the building; choosing and defining the shape of the building and its relationship with other buildings of the immediate surroundings; ordering and distributing internal spaces, considering flows and functional relationships; establishing the spatial distribution and the adequacy of the internal design of the building; defining the use of construction solutions that reduce the noise leakage; defining and applying materials that reduce the reverberation and absorption of noise; using and applying constructive details that contribute to better acoustic quality.
4.3. Smell
Such concepts bring upon reflections regarding the importance of triggering a good sense of smell within environments. In addition, how much it can interfere with the well-being of users, considering their affective memories, pleasant and unpleasant odors.
Hospital environments, according to WOSNY (2004, p.1), has its own odor. The ?smell of hospital? is indicative of quality in health and, mainly, of conditions for hospital infection.
Smells such as medicine, ?hospital food?, disinfectant, are recurrent in the statements of those who remain in the hospital, either for an elective consultation or for longer hospitalization period.
Every odor communicates something. Pleasant or unpleasant, odors send some message, obvious in various situations, in others, requiring decoding. They may mean some imminent danger present in the environment, cause or result of any damage or discomfort to the individual. The interpretation of these olfactory messages by nursing, depending on its response, can be decisive in the conduction and outcome of the act of care mediated by the relationship between olfactory perception/nursing action. It may be suggestive of physiological emanation resulting from the action of a given pathology ported by the client. Olfactory perception, sharper in one, less in others, responds to a variety of sensations. The greater aesthetic/philosophical and technical/scientific understanding of odorous fumes may favor nursing diagnosis and care planning, environmental and therapeutic quality surveillance (WOSNY, 2004, p. 1).
Some precaution should be taken when designing hospital environments, such as the choice of odorless finishing materials, place where products and medications are handled and location of the kitchen production away from patients, so as not to negatively impact the well-being of its users.
Using biophilia strategies, a topic mentioned in previous chapter, nature connects positively with man, reducing pain, stress, and anxiety. Therefore, smells of nature for hospital environments can help in the restoration of patients and the well-being of health professionals. This strategy can be carried out with an electric aroma diffuser with essential oils.
4.4. Taste
In the hospital environment, different users receive food every day. Staff, students, companions, and patients eat daily inside the hospital. Patients receive up to five meals a day. How to make this a positive experience and enhance the recovery process?
Access to a variety of safe and healthy foods is a fundamental human right. Adequate nutritional care, including food quality, has beneficial effects on patient recovery and quality of life. The presentation of the meal, the variety of products and the physical location are the primary factors that contribute to the negative perception of the user and attitudes towards the meals of institutions. Generally, the public sees hospitals as institutions, with the view that they are less favored in resources. The negative image of the hospital meal is generalized and, therefore, not necessarily related to food itself (GARCIA, 2010, p. 474).
For Hesse (2016, p.53), hospitals, in the last decade, have seen an opportunity to improve patient care, in addition to providing a competitive differential and as a way of reducing costs. In the hospital, nutrition works in an integrated manner and considers the limitations of each patient in relation to their clinical status. For him, the meal should be presented in a pleasant way, to arouse the desire to eat. In the five articles studied by Hesse, the time of hospitalization and well-planned menus are mentioned as determinant in the acceptance of hospital meal.
Hospitalized patients, either in the ICU or regular bed, receive their food in bed, often at a high table, without much ergonomics, or on a meal bench. The environment where they spend the day does not satisfactorily stimulate the taste. That is why it is so important to improve this experience with a good presentation of the meal, stimulating more than one sense.
The hospital staff or even companions, who eat their meals in cafeterias, also need adequate spaces, with coatings that absorb the noises, with the presence of real or simulated nature, with colors and stimuli that make the experience pleasant, as we can see in illustration 7.

4.5. Touch
Tieppo (2019, p.117) brings the concept of touch followed by sensitivity. By touching something, we experience not only the touch, but also sensations such as tickling, pressure, vibration or movement, temperature, pain, and position of body parts.
The sense of touch is related to human development and adaptation. It is by touching things that the baby begins to identify the different shapes and textures of objects. He also begins to understand his own body and differentiate people. People with visual impairment use their fingertips to ?read? embossed dots on a surface and orient themselves in space through touching and proprioception.
When designing hospital environments, it must be considered the touching experience to prioritize spatial reading using the Braille system, as well as use different finishing materials and furniture to make it possible to identify different places, and add other sensations to the somatosensory system, such as adequate temperature of the environment, through natural or artificial ventilation.
5. Conclusion
Bibliography
BARBEITOS, Carmo Ledna Pereira. Percepção do olfato: folhas que não guardei. 2010. Disponívelem: Acesso em 16 dez. 2021.
BRASIL. ANVISA. Agência Nacional de Vigilância Sanitária. Conforto Ambiental em Estabelecimentos Assistenciais de Saúde / Tecnologia em Serviços de Saúde. Brasília: 1ª edição, Agência Nacional de Vigilância Sanitária, 2014.
BRASIL. ANVISA. Agência Nacional de Vigilância Sanitária. Dispõe sobre o Regulamento Técnico para planejamento, programação, elaboração e avaliação de projetos físicos de estabelecimentos assistenciais de saúde. Brasília: 1ª edição, Agência Nacional de Vigilância Sanitária, 2002.
BRASIL. Agência Nacional de Vigilância Sanitária. Núcleo Técnicoda Política Nacional de Humanização. Acolhimento nas práticas de produção de saúde / Ministério da Saúde, Secretariade Atenção à Saúde, Núcleo Técnico da Política Nacional de Humanização. ? 2. ed. 5. reimp. ? Brasília: Editora do Ministério da Saúde, 2010. 44 p. : il. color. ? (Série B. Textos Básicos de Saúde).
BITTENCOURT, Fabio. Conforto acústico em ambientes de saúde. Música, paisagismo e materiais de revestimentos como soluções humanizadoras. E-book digital. Inbec Pós Graduação, 2021.
BOTTON, Alain de. A arquitetura da felicidade. Rio de Janeiro: Rocco, 2007.
CARBONE, Jessica. Guia prático. Neuroarquitetura no combate ao estresse e à ansiedade, 2021.
CRIZEL, Lori. Neuroarquitetura: neuroarquitetura, neurodesign e neuroiluminação. 1ª ed. ? Cascavel - PR: Lori Crizel, 2020.
DEBAJYOTI, Pati et al. The Impact of Simulated Nature on PatientOutcomes: A Study of Photographic Sky Compositions. 2015. Disponível em: Acesso em 10 nov. 2021. EBERHAD, John P. Applying Neuroscience to Architecture. 2009. Disponível em: . Acesso em 10 nov. 2021.
FILHO, Ruy Barbosa Soares. Resposta humana à luz: alterações não visuais e o projeto luminotécnico residencial com LEDs. 2018. Disponível em: Acesso em 13.dez 2021.
FONSECA, Pedro Ricardo Gouveia. EDWARD O. WILSON, A CRIAÇÃO. UM APELO PARA SALVAR A VIDA NA TERRA. 2009. Disponível em: http:// dx.doi.org/10.14195/0870-4112_7_29. Acesso em 13 dez. 2021.
GARCIA, Rosa Wanda Diez. Alimentação hospitalar: proposições para a qualificação do serviço de alimentação e nutrição, avaliadas pela comunidade científica. 2012.Disponívelem: Acesso em 16 dez. 2021.
JUNIOR, Hermes de Andrade. Eficácia terapêutica da música: um olhar transdisciplinar de saúde para equipes, pacientes e acompanhantes. 2018.Disponívelem: Acesso em 16 dez. 2021.
LEVITIN, Daniel J. A mente organizada. Como pensar com clareza na era da sobrecarga de informação. 1ª ed. ? Rio de Janeiro: Editora Objetiva, 2015
LEVITIN, Daniel J. A música no seu cérebro: a ciência de uma obsessão humana. 1ª ed. ? Rio de Janeiro: Editora Objetiva, 2021.
NANDA, Upali. Sensthetics: a crossmodal approach to the perception, and conception, of our environments. 2005. Disponível em: Acesso em 07 nov. 2021.
NERBASS, Flavia Baggio. Distúrbio do sono em unidade de terapia intensiva. 2015. Disponível em:<https://portal.secad.artmed.com.br/artigo/disturbios-do-sono-em-unidades-de-terapia-intensiva> Acesso em 15 dez. 2021.
PACIEVITCH,Tais. Tato. 2013. Disponível em: < https://www.infoescola. com/anatomia-humana/tato/ > Acesso em 17 dez. 2021.
PAIVA, Andrea de; JEDON, Richard. Short- and long-term effects of architecture on the brain: Toward theoretical formalization. 2019. Disponível em: https://www.sciencedirect.com/science/article/pii/ S2095263519300585#bib29 > Acesso em 08 nov. 2021.
PREUSS, Todd. How does the human brain differ from that os other primates. 2014. Disponível em: https://www.brainfacts.org/ask-an-expert/ how-does-the-human-brain-differ-from-that-of-other-primates> Acesso em 10 dez. 2021.
RAHMAN, Shadab A. Diurnal Spectral Sensitivity of the Acute Alerting Effects of Light. 2014Disponível em: https://academic.oup.com/sleep/ article/37/2/271/2558955. Acesso em 13 dez. 2021.
ROCHA, Viviane Cristina da. A música por uma ótica neurocientífica. 2013. Disponíveem: Acesso em 15 dez. 2021.
SILVA, Michelle Alves da. Visão. 2013. Disponível em www.infoescola.com/ anatomia-humana/visao/. Acesso em 12.dez.2021.
TIEPPO, Carla. Uma viagem pelo cérebro: a via rápida para entender a neurociência. 1ª ed. ? São Paulo: Editora Conectomus, 2019.
TUAN, Yi-Fu. Topofilia: um estudo da percepção, atitudes e valores do meio ambiente. Trad. Lívia de Oliveira, São Paulo: Difel, 1980.
ULRICH, Roger S. Health Benefits of Gardens in Hospitals. 2002. Disponível em: < https://greenplantsforgreenbuildings.org/news/healthbenefits-of-gardens-in-hospitals/> Acesso em 07 nov.2021.
VILLAROUCO, Vilma. Neuroarquitetura. A Neurociência no ambiente construído. Rio de Janeiro, 2021.
WOSNY, Antonio de Miranda. Odores e infecções em ambiente hospitalar. 2004. Disponível em: < https://www.scielo.br/j/tce/a/ b3rb6psBKQkCBtYwxLZdd7g/?lang=pt > Acesso em 16 dez. 2021.
ZANATA, Amanda A. et al. Biofilia: produção de vida ativa em cuidados paliativos. 2019. Disponível em: Acesso em 10 nov. 2021.


