Publications IPH Magazine Revista IPH Nº18 RECOMMENDATIONS FOR PLANNING AND CARRYING OUT RENOVATION WORKS IN FUNCTIONAL HOSPITALS
- IPH Magazine Nº18
- The therapeutic garden
- Hospital Sul América and the modern design in health architecture
- RECOMMENDATIONS FOR PLANNING AND CARRYING OUT RENOVATION WORKS IN FUNCTIONAL HOSPITALS
- How spatial syntax can help mitigate the effect of future pandemics in Brazil
- A reflection on the impact of the Covid-19 pandemic on architecture and urbanism
- Floor covering of hospital floors: Case study of the vinyl blanket applied in a hospital in Salvador, BA
RECOMMENDATIONS FOR PLANNING AND CARRYING OUT RENOVATION WORKS IN FUNCTIONAL HOSPITALS
Ramon Nascimento
With regard to As built project, NBR14645-3, of 12/2005, establishes the minimum requirements of which systems and building elements should be characterized throughout the execution of the work and after its completion, so that the owner of the building can have the record of the systems that composes its physical infrastructure (ABNT, 2005).
Abstract
Planning renovation works in operational hospital environments is a complex activity, which requires careful and a multiprofessional knowledge that goes beyond engineering, entering the spheres of nursing and medicine. With this article, we try to contribute to the dissemination of good practices in this field, through a methodology aimed at generating planning recommendations. During the investigation of the minimum care necessary for the planning and execution of renovation works and expansions of hospitals in operation, a checklist of points of attention and risk matrix was elaborated, demonstrating some actions that can be taken to mitigate critical points and guide construction staff with little experience in works within healthcare facilities. The study was based on a bibliographic survey and on an analysis of relevant standards and legislation. At the end, a number of actions are recommended for the various professionals involved in the planning and execution of works in hospitals, including the Hospital Infection Control Commission, patient-safety teams, suppliers and other workers of healthcare facilities, in order to avoid harm to patients and health organization as a whole.
Keywords: hospital planning, renovation works, risk matrix.
1 INTRODUCTION
According to Mattos (2019, p.19), the construction industry has been one of the productive branches that have presented the most significant changes in recent years. The intense competitiveness and globalization of markets, the demand for more modern goods, the increase in the emergence of new technologies, the change in the degree of demand of customers and the reduced availability of financial resources for the realization of enterprises have made business organizations realize that investing in process management and control is indispensable, because without this mechanism the enterprises lose sight of their main indicators: time, cost, profit, return on investment and cash flow.
In the case of investments in Health Care Facilities (EAS), mainly in renovations and expansions of hospitals that are in operation and cannot stop their operations, it is necessary to apply planning tools that help reduce their impacts, which can range from safety of patients, decrease in hospital unit revenue, dissatisfaction of building users, poor application of investments, among other risks inherent to the absence of a correct and continued planning.
This research aims to contribute to the dissemination of good practices, guidelines and minimum care that are necessary for the planning and execution of renovation works and expansions of hospitals in operation, through the preparation of a checklist of points of attention and a matrix of risks, demonstrating some actions that can be adopted to mitigate critical points and guide the teams of professionals working withing healthcare facilities.
2 LITERATURE REVIEW
2.1 Project lifecycle
An engineering enterprise must be developed following a logical sequence of development of the final product, carrying out its phases in feasible time to achieve the objectives outlined for each phase, generating products that will lead to the further sequential phases (MATTOS A. D., 2019, p. 27).
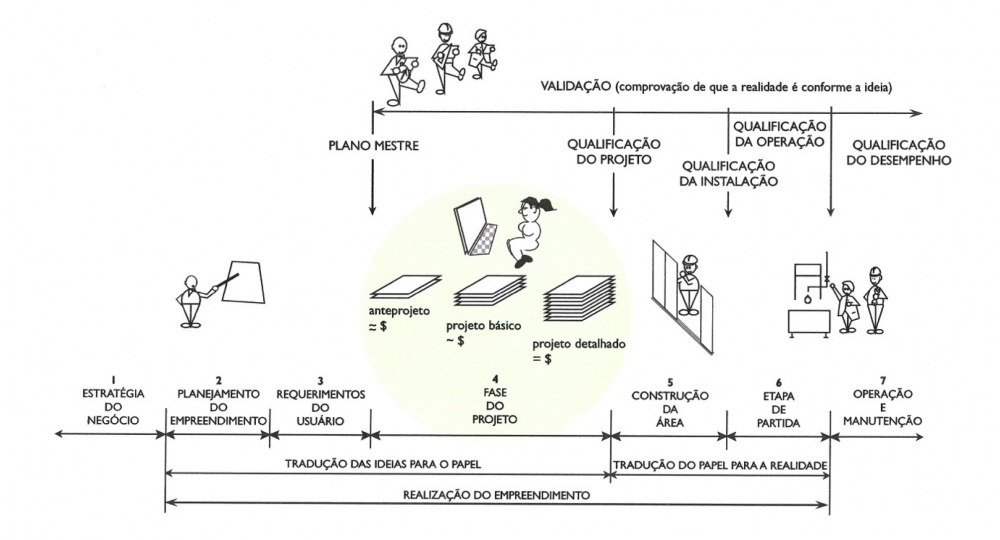
The different phases of an enterprise, from its conception to execution are presented in the image below, in which are indicated the milestones that professionals in the sector use to measure the evolution of the project and construction. For example: preliminary design, basic design and detailed design (SBCC: Working Group GT 4, 2012, p. 17).
Image 1 - The project in the business life cycle
Source:
SBCC - Working Group, GT 4, 2012
The intervention stages include: elaboration of the Strategic Masterplan, the Hospital Physical Masterplan, Management of the Building Documentation, and the Planning and Elaboration of Projects, reaching the Contingency Plan and the Execution of the work itself, from which the Commissioning takes place, followed by further steps after the execution, such as the elaboration of As Built projects and the Manuals of Use, Operation and Maintenance, as we will see in the following points.
2.2 Strategic master plan
In the strategic scope, any investment action in a health enterprise, whether a renovation or an expansion, should be the result of strategic planning, since "healthcare buildings are living organisms in constant adequacy to the strategy of the companies which occupy them'' (BROSS, 2013, p. 196).
The core of strategic planning is how to answer the following questions: What to do to achieve the objectives set by the institution? How to develop the steps, aiming to achieve the desired purpose? When to trigger actions in this direction? How to generate a favorable future with the objectives outlined? (PEREIRA & GALVÃO, 2005, p.73).
The core of strategic planning is the first step towards the elaboration of a Master Plan, clearly establishing the reason for the existence of the healthcare facility, because all institutions must initially have a reason for being, an objective or an institutional mission, which is a kind of operational summary of its nature and its central values, synthesized from the following points: what it does, why it does it, where it does it, for whom it does it, and how it does it (BADERMANN DE LEMOS, 2017, p. 9).
2.3 Hospital Physical Masterplan
Also in the planning context, the hospital physical masterplan aims to diagnose the existing physical infrastructure and define its potential for use, for a long period, and should be flexible enough to adapt to the needs of future change, in a structured enough way for financial decisions to be made, also providing for the needs of reforms and expansions according to the execution in phases, in order to organize circulations and connections with new works, demonstrating the sectorization of the units and the changes envisaged in each stage (MENDES, 2018, p. 90).
In this context, the hospital physical masterplan becomes an indispensable part in the planning of the organization, being fundamental for the physical-functional reorganization of an existing hospital and, in the development of an architectural project of a new hospital, serving as a device for defining the types of interventions to be proposed, based on the existing capacity of the existing physical infrastructure and the perception of projections care demands (LEMOS, 2017).
The absence of medium and long-term planning will result in invisible pseudo savings, which will affect the future performance of the institution and, when it cannot be directly measured, for example, may prevent a new imaging diagnostic unit from being deployed in the hospital as a result of the recent implementation in the same location, a warehouse and a laundry unit (MADRIGANO, 2006, p. 9; CARVALHO, 2014, p. 65) .
2.4 Document management of the building
Another essential item for planning and executing renovations and expansions in healthcare facilities is the document management of physical infrastructure. Particularly in health buildings, it is essential to keep projects constantly updated and compatible (BITENCOURT & COSTEIRA, 2014, p. 46), and this care with the document management of the building is not only a good practice, but a matter of safety of the patient and users of the building.
The availability of the project on site is mandatory, as provided for in RDC No. 189/ANVISA, which establishes in Article 5th that " the owner must keep filed in conjunction with the project approved by Sanitary Surveillance in the topics related to complementary projects of structures and facilities, when it fits, as provided for in item 1.3 of the resolution" (ANVISA, RESOLUTION - RDC No. 189, 2003), summing up this determination through RDC No. 63 of 2011 in Article 23rd which says:
"...the health service must keep available, according to its type of activity, documentation and registration referring to: I - Basic Architecture Project, approved by the competent Sanitary Surveillance." [...] VII - Preventive and corrective maintenance of the building and its facilities" (ANVISA, RESOLUTION-RDC No. 63, 2011).
2.5 Planning and projects
After having defined which works and renovations will take place in the healthcare facility with the respective physical-functional programs of all units/environments to be deployed and/or renovated, the institution can start the development of technical architectural and engineering projects safely (MADRIGANO, 2006, p. 69).
After defining the scope of the project, the feasibility studies for the project are initiated. This is the phase when investors study its feasibility and make the estimative of costs, as noted by Nascimento (2015):
"The great importance of a cost estimate lies in making feasibility analyses of the project, allowing choices of alternatives to be adopted in the detailing stage of the projects, without fixing the high burden of preparing a budget" (NASCIMENTO, 2015).
It is observed that the advantage of conducting a good feasibility study is clear when compared to the possible costs of making changes during the phases of design and construction.
Another point to be taken into account before the decision-making, during planning and designing phases, is related to hospital infection control, which can be carried out through studies of the risk control, aiming to integrate infection control and epidemiology into the planning process of hospital infrastructure projects and enabling, through this planning tool, the early mapping of risks to patients, as well as the identification of possible interruptions of essential services for patients (COUTO, R.C, 2009, p. 363).
Therefore, an inadequate analysis of the risks of dissemination of hospital infection will possibly result in failure in the definition of precautionary barriers to control hospital infection in the area of the work and in its immediate surroundings. The lack of financial resources for the correct sealing of passage areas, with the installation of sidings and other elements, can cause problems during the execution of the work, which can be avoided if such elements are foreseen since the phase of project development (PADULA, 2017).
2.6 Contingency Plan
Concomitantly with the planning of architectural and engineering projects, the elaboration of the contingency plan aims to map the risks involved in the execution of the work, as well as to define people who will be responsible for acting before, during and after its execution (1).
According to Padula (2017), Ribeirão Preto Medical School's Hospital das Clínicas, University of São Paulo HCFMRP - USP, outlined a contingency plan encompassing several actions to predict, avoid or mitigate risks, as well as to improve the understanding of all parties involved in the project of the work or renovation (PADULA, 2017).
| ITEM | SHARE | OBJECTIVE |
| 1 | Appointment of the Project Administrative Manager | Represented by a technical advisory server, this professional is assigned to all projects where there is the possibility of direct or indirect interference in care, its main tasks are: to give science to all areas involved in the project; to participate and monitor the entire process of planning and execution of the work, in order to ensure, before the Engineering Division, that the contractual requirements with the expected quality are met; establish the systematized monitoring of the work or renovation, in order that potential setbacks or deviations from compliance with the actions provided for in the Manual are identified in advance and reported to the Administration. |
| 2 | Manual of Planning and Monitoring of Works | Describe the attributions and actions to be developed by each of the areas involved in the construction projects. |
| 3 | Risk Assessment | Bring more clarity to the definition of the barriers of precautions against hospital infection to be used in each work. Make possible the specification and prior allocation of the necessary financial resources to be foreseen in the budget worksheet of the work.
|
| 4 | Preparation of two checklists verification and the Term of Responsibility | Form to be delivered to the company that is the winner of the execution of the work. Developed from the content of the Monitoring Manual, these instruments aim to give science and systematize the evaluation of compliance with actions, which ensure the quality and safety of the performance of the care activities of the area under construction, and those of its surroundings. |
Table 1 - Actions adopted by HCFMRP - USP for contingency of works
Source: PADULA, 2017 - adapted by the author
It is observed that the strategy adopted by HCFMRP-USP gave great importance to the concepts about flows in the preparation and approval of projects of renovation works, in addition to considering the regulations and good practices adopted by the organization for the execution of the works and their respective phases; the obligations of the contracted company; the particularities for carrying out works with the hospital in operation; greater understanding and commitment of the parties involved, during the execution of the work with regard to the risks of hospital infection; better control of access of people in the work; improvement in signalization, hygiene, transportation, disposal of debris and implementation of protective barriers in the area under construction (PADULA, 2017).
2.7 Execution of the work
When carrying out works in functional hospitals, it will not always be possible to carry out construction or renovation activities as planned and within the desired time, which is why it is essential to plan them in advance to reduce their interference in daily hospital activities. It should be taken into account, in this process, that there are still few companies specialized in hospital works, which is why it must be ensured that it is clearly transmitted to all the actors in the construction all information concerning hospital environment specific standards and rules (ANVISA, HOSPITAL SAFETY).
In this context, some ABNT rules already bring some points to be followed regarding good practices in the execution of hospital works, such as:
- NBR7256 of 03/2005 - Air treatment in healthcare facilities - Requirements for design and execution of facilities.
- NBRISO14644-4 of 04/2004 - Clean rooms and associated controlled environments - Part 4: Design, construction and start-up.
- NBR12188 of 03/2016 - Centralized systems for the supply of medicinal gases, gases for medical devices and vacuum for use in health services.
- 10/2017 NBR 13587 - Health Service - Oxygen Concentrator System (SCO) for use in centralized medicinal oxygen system - Requirements.
- NBR16651 of 04/2019 - Fire protection in health care facilities (EAS) - Requirements.
Based on these regulations, we highlight on Table 2, below, some of the main points of attention related to protocols to be adopted during the execution of works and renovation in healthcare facilities and controlled environments:
| ITEM | REGULATION | STANDARD OF THE WORK |
| 1 |
NBR7256 of 03/2005 Air treatment in health care facilities (EAS) - Requirements for design and execution of facilities |
6.3.7 Construction
[...]
6.7.3.7 - Maximum care must be taken during assembly to keep the inner surface of the ducts clean; the ducts must be manufactured in a clean environment, carefully cleaned internally, capped on both sides and taken to the assembly site where they will be opened on one side and connected to the stretch already installed, and so on. It should be ensured that internal cleaning of the installed ducts is maintained.
|
| 2 |
NBR12188 of 03/2016 Centralized systems for the supply of medicinal gases, gases for medical devices and vacuum for use in health services |
4.11.1.13 Before installation, pipes, valves, joints and connections must be properly cleaned of oils, greases and other combustible materials, according to CGA G-4.1.
4.44.1.14 After cleaning, special care should be taken when stocking and handling this material in order to avoid recontamination prior to final assembly.
4.11.1.15 Pipes, valves, joints and connections shall be closed, buffered or sealed to prevent foreign objects from penetrating them until the moment of final assembly.
4.11.1.16 During assembly, segments that have remained incomplete must be closed or buffered at the end of the working day.
4.11.1.17 The tools to be used in the assembly of the plant and terminal distribution network must also be free of oil and grease.
|
| 3 |
NBR16651 04/2019 Fire protection in healthcare facilities - Requirements |
11 Requirements for renovation and expansion
11.3 General requirements
11.1.3 The intervention phases shall be properly planned in order to avoid obstruction of emergency exits. If the original emergency exits are temporarily obstructed during the intervention, alternative escape routes and exits should be provided for each phase of the intervention.
|
Table 2 - Points of attention in ABNT concerning specific standards for healthcare facilities
Source: ABNT- adapted by the author
2.8 Commissioning
The commissioning phase is the result of an entire process, which aims to ensure that the systems and components of a building or industrial plant comply with the requirements and operational needs of the customer, concerning its design, installation and testing of operation.
(SGS, 2018).
In this context, ABNT standards provide for some points of attention to be followed regarding the commissioning of the healthcare facility physical infrastructure, such as:
| TEM | REGULATION | REGULATION HIGHLIGHTS CONCERNING THE COMMISSIONING OF THE WORK |
| 1 |
NBR7256 of 03/2005 Air treatment in healthcare facilities - Requirements for design and execution of facilities |
7. Commissioning of facilities
[...] 7.4 Site delivery report
A report detailing the procedures adopted, with the record of the results of all tests and measurements performed, should be prepared in accordance with ABNT NBR 10719. The report shall certify that the installations have been designed and executed in accordance with the requirements of this Standard and shall be approved by the supervision of TAB Services and supervision agents.
|
| 2 |
NBR12188 of 03/2016
Centralized systems for the supply of medicinal gases, gases for medical devices and vacuum for use in health services
|
5. Test for commissioning of the installation of the centralized system
[...] 5.1 After the installation of the centralized system, the network must be cleaned with medicinal air and tests shall be carried out in accordance with 5.1.1 to 5.1.10.
[...] 5.1.10 These tests shall be carried out in the presence of a representative of the health service, who shall sign the test report together with the assembler and shall keep, in its archives, the updated designs and designs of the gas and vacuum distribution networks.
|
| 3 |
NBR13534 of 01/2008
Low voltage electrical installations - Specific requirements for installation in health care facilities
|
7. Final check
7.102 In addition to the requirements contained in Section 7 of ABNT NBR 5410:2004, the facilities covered by this Standard shall be subject to verifications 1) to 5) below. Checks must be carried out prior to installation and replacement of the installation, i.e., after deployed and after any change or repair:
|
Table 3 - Points of attention in ABNT concerning specific standards for healthcare facilities Source: ABNT, adapted by the author
It is observed that commissioning must be carried out in all phases of the enterprise, from the project phase to the delivery of the enterprise, being generally executed in the construction and assembly phase, thus avoiding failures and difficulties in the operation and maintenance of industrial plants after the complete installation (SGS, 2018).
2.9 As built and Manuals of Use, Operation and Maintenance
The quality of the technical documentation, elaborated during the phases of design and execution of the work, and its direction to elucidate issues related to the stages of conservation, use and maintenance, and the operation of the equipment in a systematized way, in the form of manuals, has been an instrument to improve communication in the process (ABNT, 2011).
With regard to As built project, NBR14645-3, of 12/2005, establishes the minimum requirements of which systems and building elements should be characterized throughout the execution of the work and after its completion, so that the owner of the building can have the record of the systems that composes its physical infrastructure (ABNT, 2005).
With regard to the building manuals, NBR 15575-1:2021 establishes it is up to the builder and developer to prepare the manual for the use, operation and maintenance of the building, also following the requirements set out in ABNT NBR 14307, which details the warranty deadlines applicable to the various construction systems (ABNT, 2021).
All this pack of documentation on the physical infrastructure of the hospital will serve as a basis for future maintenance and conservation actions of the building, as well as for possible further interventions for renovations and expansions, assisting in the identification and mitigation of risks, as well as saving time during the decision-making phases of projects (BITENCOURT & COSTEIRA, 2014, p. 46).
3 METHODOLOGY
To achieve the overall objective of this research, we framed the following strategy:
- To assess, through a bibliographic survey, what are the good practices adopted for planning and execution of works in operational hospitals;
- To prepare a checklist with the main points of attention to be observed when planning works in healthcare facilities;
- To validate the checklist with points of attention, after being verified with experts and companies that plan and carry out works at healthcare facilities;
- To develop a risk matrix (2) risks based on the checklist, demonstrating the actions to be taken to prevent and mitigate negative events during expansion and renovation works in healthcare facilities.
(2) [...] the risk matrix is a tool that allows managers to measure, evaluate and order risk events that may affect the achievement of the objectives of the unit. [...] A risk matrix is a tool that qualitatively classifies impact and probability weights. [...] In general, risk events located in the quadrants defined as high risk and critical risk are generally considered indicative of the need for stricter
During the bibliographic survey, we referred to references of planning and control of works, such as those from Aldo Dórea Mattos (MATTOS A. D., 2019), as well to Guia para Projetos de Áreas Limpas, by Brazilian Society of Contamination Control - SBCC (SBCC: Working Group GT 4, 2012), which addresses the planning of works in controlled environments. Based on these literatures, the general scope of the checklist was elaborated.
During the literature review, we also consulted other authors and technical standards of ABNT that approach generally or specifically themes related to: Strategic Masterplan; Hospital Physical Masterplan; Building Management Documentation; Planning and Projects; Contingency Plan; Work Execution; Commissioning; As Built; and Manuals of Use, Operation and Maintenance; all topics related to the planning and execution of works in healthcare facilities, as shown in Image 10.
We also highlight that regarding the Contingency Plan, we referred to bibliographic sources in the area of nursing and infectology, since this theme is transversal to health care activities and physical infrastructure of healthcare facilities.
Therefore, once the macro themes of the check list were structured, we consulted in the bibliographic references the points considered to be more relevant to be observed in the act of planning and carrying out works in a functional hospital and, then, we sought advice from professionals working in the planning and/or execution of hospital works, in order to validate whether the themes identified as a point of attention are relevant.
One the checklist was validated, we framed a risk matrix, pointing out the impacts and actions to be carried out in order to mitigate or avoid damage, during the planning and execution of works, being consulted a specialist in risk management to guide the model adopted.
As for the methodology adopted for the elaboration of the risk matrix, we used as a reference the Risk Matrix Guide of the Ministry of Planning, Development and Management; and as a scope of this matrix, the macro divisions proposed in the points of attention checklist.
controls, while risks located in the small and moderate risk quadrants would be indicative of more moderate controls. It also points out that in some cases there would be no need to implement controls and/or even remove controls (MINISTRY OF PLANNING, DEVELOPMENT AND MANAGEMENT, 2017).
4 RESULT AND DISCUSSION
Based on the research carried out, it was found that, in order to plan a health enterprise, design it and, in particular, carry out works in operational hospitals, it is necessary to have a multidisciplinary team including engineers, architects, healthcare professionals, administrators, suppliers and other necessary actors.
In addition, it was observed that, in order to obtain good results in the execution of works in a hospital environment, it is essential to have a well-organized health institution, with business strategy, risk assessment, hospital physical master plan, infection control plan, contingency plan, building document records and well-designed architectural and engineering projects.
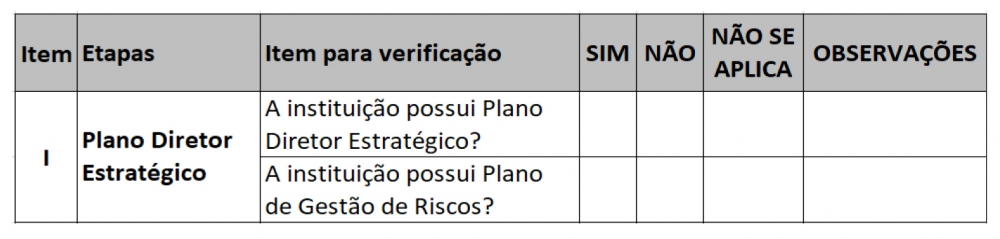
Based on the macro steps defined, the checklist and the risk matrix were elaborated, with points of attention that must be assessed during the planning and execution phase of works in operational hospitals. Such points were validated with experts from the field; the checklist began at the macro stage of Strategic Masterplan, then we developed the risk matrix, highlighting the relevance of the points of attention raised (see Tables 2 and 3).
Table 2 - Checklist: Point of attention - Strategic Masterplan
Source: from the author himself
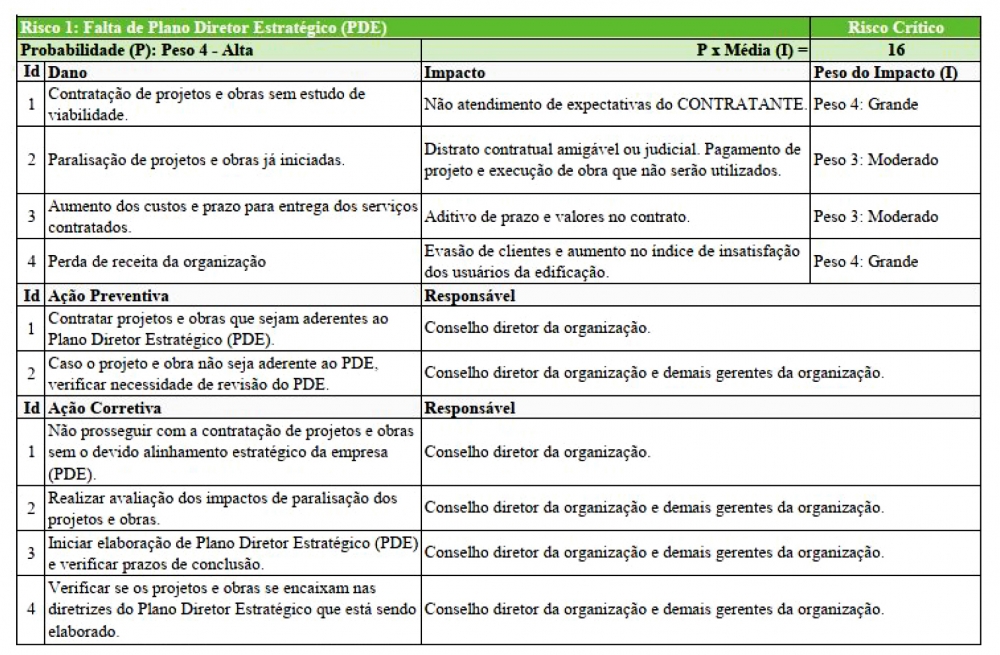
Table 3- Risk Matrix - Risks1 and 2: lack of strategic planning
Source: from the author himself
Based on the points of attention exposed in the checklist and the risk matrix, it was observed that, without proper strategic planning for decision making, to know when and how to start an investment in renovation and expansion works in the hospital, with or without a risk management policy, with an established committee and with elaborate risk map, the decision to be taken (3) becomes fragile and, consequently, the feasibility study of the inaccurate undertaking, which may cause conflicts and complications in the participation of the actors of the work, "[...] the future is uncertain and cloudy when senior management seems to start each day with a blank sheet of paper, without a planned continuity of actions" (PEREIRA & GALVÃO, 2005, p. 74).
As for the hospital physical masterplan, it was verified that it is a very effective strategic tool for forecasting future investments in health organization works, which contributes to mitigate risks in the institution's investments and stakeholders. From this context, the main points of attention were described in the checklist and in the risk matrix for the Hospital Physical Masterplan.
(3) The risk map should be continuously updated, as the project progresses, some risks can be eliminated with the completion of certain activities, other risks may be reduced and new risks may arise. Therefore, risk management is an activity that should be terminated only after the completion of projects" (BARRAL, 2021).
Thus, it is concluded that, while the costs of renovation are high, especially in long-time neglected buildings, and as there is usually little resources available, there is a willingness to spend first on aesthetic work, but it is essential that the most critical interventions are made before cosmetic work (MENDES, 2018, p. 100) , so the hospital physical masterplan will be the basic tool to prevent resources from being applied in works that are actually pseudo savings.
As for the building management documentation, it was noticed throughout the research that this should be the basis for planning future works in a hospital unit, and that the projects as built and the manual of use, operation and maintenance will directly impact both the management and technical decision-making and the phase of implementation of the business strategy. Thus, the inexistence of such physical infrastructure documentation may imply the following problems: [...] "carry out operations in the various facilities without an accurate mapping of their distribution; [...] depend on the memory of former employees or exchange complete systems of facilities for lack of a correct survey of their distribution" (BITENCOURT & COSTEIRA, 2014, p. 46).
Once established what to do, why doing it, where to do it and for whom to do it, comes the part of planning and elaborating architecture and engineering projects, which will fit the what to do, and should be developed within the technical premises of the various technical
regulations of ABNT and ANVISA, following the basic stages of project development: preliminary study; preliminary project; basic project; and executive design. Such stages are defined in NBR16636 - Preparation and development of specialized technical services of architectural and urban projects.
With regard to the contingency plan, during the bibliographic review, it was identified as an essential macro step, since the planning phase serves to map the inherent risks, such as those related to hospital infection associated with the work being carried out. It is at this stage that decisions are made for possible relocations of patients, partial or total interruptions of care services.
As for the point of execution of works in functioning hospitals, little was found of specific engineering literature on the subject, being more addressed in the field of nursing and infectious diseases, besides in some specific norms of ABNT, that deal with building systems of healthcare facilities and, occasionally, in other standards that deal with buildings in general.
It was also verified, throughout the research, that the issues related to patient safety and hospital infection control are intrinsic to the work, so such precautions do not affect only patients, but the system of the land. In addition, it was found that the main measures related during the execution of the work are related to precautions related to construction sites.
As for the stages as built and manual of use, operation and maintenance, it was observed that such documentation is essential for the final phase of the work, and should be carried out and updated throughout the execution of the work to maintain the traceability of what is being built and acquired.
With regard to commissioning, throughout the research, it was observed that it is not enough to build the work, but it must also be tested and validated in order to be verified whether the construction was carried out according to the project requirements, assessing safety through tests and reports that will attest the building can be put into use and operation.
All these steps aim to avoid economic damage to health organizations, material damage to buildings and its users and, consequently, damage to the health of patients, who seek hospital buildings to heal themselves.
5 FINAL CONSIDERATIONS
The initial impression on the subject led us to believe it would be a simple task to sum it up, however when researching it more thoroughly, a range of essential information was observed that would not fit in the few pages that an article supports, especially when considering the multidisciplinary nature of the theme.
It is notorious that, in hospitals, as well as in healthcare facilities in general, works are very common, and most of these places are always under renovation, in search of better serving the user getting more market share in the health market. Thus, it is recommended to all professionals involved in the planning and execution of works in hospitals that faithfully follow the provisions of the established technical standards, as well as seek to include, throughout the entire planning of such works, health professionals, patient safety teams, suppliers, and others hospital workers to avoid or minimize harm to patients and to the health organization as a whole.
REFERENCES
ABNT. (12 de 2005). NBR14645-3 Elaboração do "como construído" (as built) para edificações - Parte 3: Locação topográfica e controle dimensional da obra - Procedimento.
ABNT. (07 de 2011). NBR14037. Diretrizes para elaboração de manuais de uso, operação e manutenção das edificações - Requisitos para elaboração e apresentação dos conteúdos. Rio de Janeiro, RJ: ABNT.
ABNT. (12 de 2017). NBR 16636-1. Elaboração e desenvolvimento de serviços técnicos especializados de projetos arquitetônicos e urbanísticos - Parte 1: Diretrizes e terminologia.
ABNT. (03 de 2021). NBR15575-1. Edificações habitacionais - Desempenho - Parte 1: Requisitos gerais.
ANVISA. (18 de JULHO de 2003). RESOLUÇÃO - RDC Nº 189. Regulamentação dos procedimentos de análise, avaliação e aprovação dos projetos físicos de estabelecimentos de saúde no Sistema Nacional de Vigilância Sanitária, altera o Regulamento Técnico aprovado pela RDC nº 50, de 21 de fevereiro de 2002 e dá outras. Brasília, DF, Brasil. Fonte: http://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2003/res0189_18_07_2003.html
ANVISA. (25 de NOVEMBRO de 2011). RESOLUÇÃO-RDC Nº 63. Requisitos de Boas Práticas de Funcionamento para os Serviços de Saúde. Brasília, DF, Brasil. Fonte: https://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2011/rdc0063_25_11_2011.html
ANVISA. (s.d.). SEGURANÇA NO AMBIENTE HOSPITALAR. Acesso em julho de 2021, disponível em www.anvisa.gov.br
BADERMANN DE LEMOS, J. (Setembro de 2017). Planos Diretores para hospitais nos dias de hoje. Revista IPH - Nº 14. Fonte: https://www.iph.org.br/revista-iph/materia/planos-diretores-para-hospitais-nos-dias-de-hoje
BARRAL, R. (4 de Julho de 2021). Entrevista informal: Gestão de Risco. (R. N. Sousa, Entrevistador) Brasília, Distrito Federal, Brasil.
BITENCOURT, F., & COSTEIRA, E. (2014). Arquitetura e Engenharia Hospitalar: Planejamento, projetos e perspectivas. Em A. P. Carvalho, Coordenação de Projetos de Estabelecimentos (1 ed., p. 394). Rio de Janeiro, RJ: Rio Books.
BRASIL. Ministério da Integração Nacional. Secretaria Nacional de Proteção. (2017). Módulo de Formação: Elaboração de Plano de Contingencia - Livro Base. Brasília, DF, Brasil. Fonte:https://antigo.mdr.gov.br/images/stories/ArquivosCivil/ArquivosPDF/publicacoes/II---Plano-de-Contingencia---Livro-Base.pdf
BROSS, J. C. (2013). Compreendendo o Edifício de Saúde (Vol. 2). São Paulo: Atheneu.
COUTO, R. C. [et al]. (2009). Infeção Hospitalar e Outras Complicações Não-Infecciosas da Doença - Epidemiologia, Controle e Tratamento (4 ed.). Rio de Janeiro, RJ, Brasil: Guanabra Koogan.
CARVALHO, A. P. (2014). Introdução à Arquitetura Hospitalar. Salvador: GEA-hosp.
MADRIGANO, H. (2006). Hospitais: modernização e Revitalização dos Recursos Físicos: Manual do administrador. (G. Koogan, Ed.) Rio de Janeiro, RJ, Brasil: Editora Lab.
MATTOS, A. D. (2019). Planejamento e controle de obras (2 ed.). São Paulo, SP, Brasil: Oficina de Textos.
MENDES, A. C. (2018). Plano Diretor Físico Hospitalar: Uma Abordagem Metodológica Frente a Problemas Complexos (1 ed.). Londrina, PR, Brasil: Kan.
MINISTÉRIO DO PLANEJAMENTO, DESENVOLVIMENTO E GESTÃO. (07 de 06 de 2017). Matriz de Riscos. Matriz de Riscos-Gestão da Integridade, Risco e Controles Internos da Gestão, 1.1 . Brasília, DF, Brasil. Fonte: https://www.gov.br/infraestrutura/pt-br/centrais-de-conteudo/170609-matriz-de-riscos-v1-1-pdf
NASCIMENTO, R.. (2015). Estimativas e custos na construção de edificação para estabelecimento assistencial de saúde (eas) no âmbito de rondônia. São Paulo, SP, Brasil.
PADULA, K. M. (2017). Gestão da qualidade e da segurança em obras e reformas nas Instituições Hospitalares. A experiência do Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (HCFMRP USP) frente a este desafio. Revista QualidadeHC. Access in July 2021, available at https://www.hcrp.usp.br/revistaqualidade/Pesquisa.aspx
PEREIRA, L. P., & GALVÃO, C. R. (2005). Administração hospitalar: Instrumentos para gestão profissional. São Paulo, SP, Brasil: Loylo.
SALES, M. D. (20 de Janeiro de 2010). Capítulo 5 - Aspergilose: do diagnóstico ao tratamento. Scielo Brasil: Jornal Brasileiro de Pneumologia. Fonte: https://www.scielo.br/j/jbpneu/a/8yMyT3zYFm3TRTbc7JBmrrR/?lang=pt
SBCC: Grupo de Trabalho GT 4. (2012). Guias para Projetos de Areas Limpas: em acordo com a norma NBR ISO 14644. Sao Paulo, SP: SBCC - Sociedade Brasileira de Controle de Contamina.
SGS. (ABRIL de 2018). COMISSIONAMENTO, O QUE É PRECISO SABER? UMA DISCUSSÃO CONCEITUAL SOBRE COMISSIONAMENTO E SUAS APLICAÇÕES. Fonte: https://www.sgsgroup.com.br/-/media/local/brazil/documents/white papers/industrial/sgs-ind-commissioning-pt-brazil.pdf
Share




Send by e-mail: